Blog Post
- Amanda Sheehan, DDS: “Do Your Implant Patients Need a Bite Splint?”
Magazine Articles
- Ken Berley, DDS, J.D., and Jesse Teng, DDS: "Why Every Dentist Must Screen for Sleep-Related Breathing Disorders"
800-854-7256 USA
Dr. James Boyd discusses the NTI-tss Plus and its positive effects on migraine sufferers.


Headaches and migraines have a devastating effect on quality of life — and for some people, these conditions occur weekly or even daily.
Migraines are the third most prevalent illness in the world and is the primary cause of disability in the under-50 age demographic. In the U.S., migraines affect 18% of women (about 28 million) and 6% of men. Approximately half of female migraine sufferers will experience more than one attack per month. More than 157 million workdays are lost annually due to migraines.
Patients are often presented pharmacological solutions to cope with their headaches and migraines. While these may work for some initially, patients should be wary of long-term use of pain medication because of the cost, side effects and risk of developing dependency. To combat these negative aspects of migraine pills, one dentist, Dr. James Boyd, created a new solution to help prevent migraines.
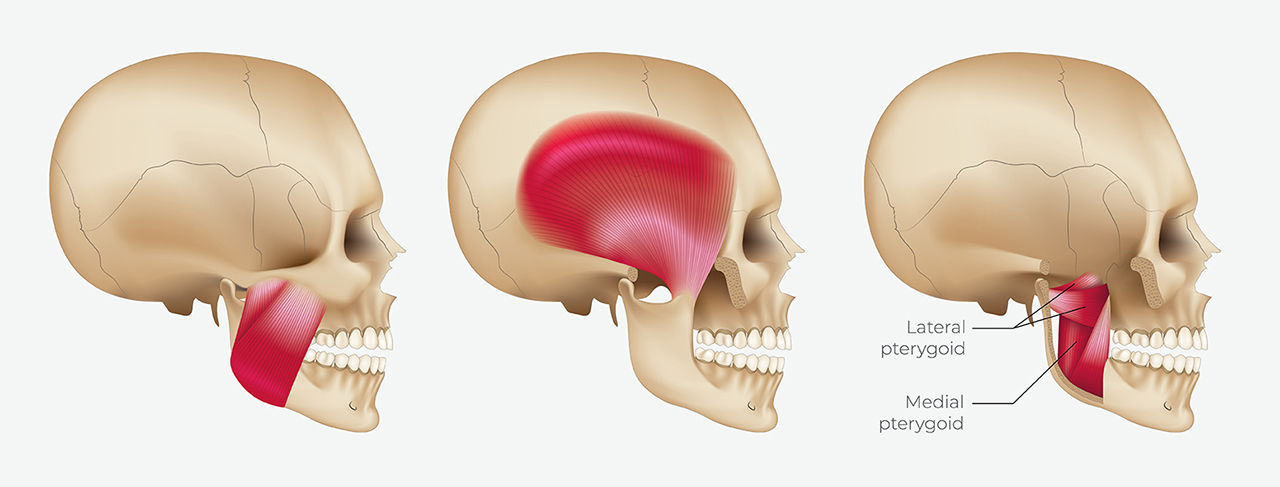
The NTI-tss Plus® is a simple anterior point-stop discluding device that reduces the maximum clenching power of the muscles of mastication by approximately 70%. The nociceptive input produced by the over-activity of these muscles, specifically the temporalis, has been found to be a significant contributor to headaches and migraines.
The NTI-tss Plus therapeutic protocol has proven to be the most effective dental pathway to treat migraines. Its efficacy has been demonstrated to be comparable to widely prescribed pharmacological treatments without unwanted side effects. In an FDA clinical trial, 82% of individuals diagnosed with migraines experienced a 77% reduction in migraine events when using the NTI-tss Plus.
Dr. James Boyd sat down with the team at Glidewell to explain more about how the NTI device was developed.
Randy Clare: Who was your first patient for the NTI, and what problem were you trying to solve when you initially envisioned the solution we now know as the NTI-tss Plus?
Dr. James Boyd: I was actually my first patient. I had been waking up with a headache every morning for 12 years. For the last four of those years, I was wearing a balanced flat-plane splint with canine rise. That didn’t do anything to stop me from clenching with full force. To the contrary, it provided a flat surface to clench into, which actually increased the intensity and frequency of my migraines.
I recalled a lecture where it had been suggested that placing a midline anterior point stop on the splint to get someone out of acute muscular distress could be very helpful as long as you remove the point stop after a few days. If it was so effective for the relief of acute pain, I wondered why it wouldn’t help my chronic headaches.
So, I added what I called a “discluding element” to my splint and experienced almost immediate relief the next morning. This concept evolved into what thousands of dentists now know as the NTI therapeutic protocol.
RC: From a clinical perspective, how does the NTI work to prevent migraines?
JB: The primary goal in migraine prevention is to minimize as much nociceptive input to the trigeminal sensory nucleus as possible. Migraine attacks are the result of trigeminal sensory “dysmodulation,” thought to be caused or enhanced by regular nociception. With the third division of the trigeminal nerve being the biggest conduit of nociception, the reduction of clenching intensity and the excessive strain and load it creates in the joints and teeth has been shown to be one of the most effective methods of reducing migraine activity.
RC: How does bruxism figure into the practice of migraine therapy, and how should clinicians explain migraine triggers to their patients?
JB: Bruxism, or teeth grinding, occurs when teeth are in occlusion, and alternating lateral pterygoid activity causes side-to-side movements. For bruxism to occur, the mandible must first be elevated (the clenching component), the teeth in occlusion, and the masseters and temporalis contracting.
The intensity and persistence of the clenching dictates the degree of resistance encountered by the lateral pterygoids as they attempt to move the mandible, or the grinding component. When clenching intensity is at a minimum, grinding movements are fluid and minimally destructive. As clenching intensity increases, grinding becomes more restrictive and strenuous. When clenching intensity reaches pathologic levels, teeth and restorations are damaged. In many cases, grinding becomes impossible. If, at that moment, the mandible is not in a centered position, the degree of nociception is increased still further.
Everyone’s physiology is unique, and different stimuli can trigger a neurological event like a migraine. Eliminating one of these triggers can decrease the likelihood of initiating a migraine. The NTI-tss Plus minimizes chronic nociception, thereby reducing the sufferer’s susceptibility to their triggers and the severity of attacks.
RC: Why would a dentist choose an NTI over another splint?
JB: The goal in splint therapy is twofold. First, splint therapy is designed to minimize muscular activity. Second, it’s designed to minimize the strain, load, and physical damage to teeth and joints. A traditional splint cannot minimize clenching intensity. In fact, traditional splints can increase clenching intensity.
Joint strain and load occur in excursive movements with posterior contact. A dentist must ensure that there is immediate posterior disclusion in excursive movements with the traditional splint. However, that can only happen when the patient is clenching on the splint and the patient is in an excursive movement. The NTI-tss Plus provides full-time posterior disclusion in a centric clench and when any excursive movements are taking place. This instant and continual incisal guidance has been shown to reduce temporalis contraction intensity by approximately 70%.
RC: When shouldn’t a dentist use an NTI?
JB: If the sole goal is to prevent teeth from being worn and the patient is an asymptomatic bruxer, another splint will suffice. For headache and migraine sufferers, the NTI-tss Plus is the ideal solution.
RC: Is the NTI for long-term use or only short-term wear?
JB: The NTI Therapeutic Protocol can certainly be used for both short-term and long-term use. As long as the signs and symptoms of nocturnal parafunction are present, then an NTI is indicated.
Some dentists worry that posterior supraeruption may occur due to long-term use; however, the alveolar stimulation that occurs during the 16 hours when the patient isn’t wearing the NTI is enough to prevent any supraeruption. Studies have shown that it takes eight consecutive days of disclusion for any supraeruption to occur.
Another misguided concern is that anterior intrusion can occur with long-term NTI use. This is simply unfounded. Some think that the forces being concentrated in the anterior can intrude the incisors opposing the NTI discluding element. The NTI, however, reduces those forces by 70% or more, which is far less than the force required to intrude teeth.
RC: Some think of the NTI as a splint that only covers the anterior teeth. What makes an NTI an NTI?
JB: The “NTI therapeutic protocol” stipulates that the discluding element evenly contacts the opposing midline while discluding the canines and posterior teeth in a centric clench and during all bruxing excursions while also maintaining minimal vertical dimension (thereby minimizing condylar rotation). A pivotal FDA clinical trial concludes that 82% of the participants using the NTI-tss device had an average 77% reduction in migraine events after eight weeks of use, and 16% experienced an 85% to 100% reduction of headache events overall.
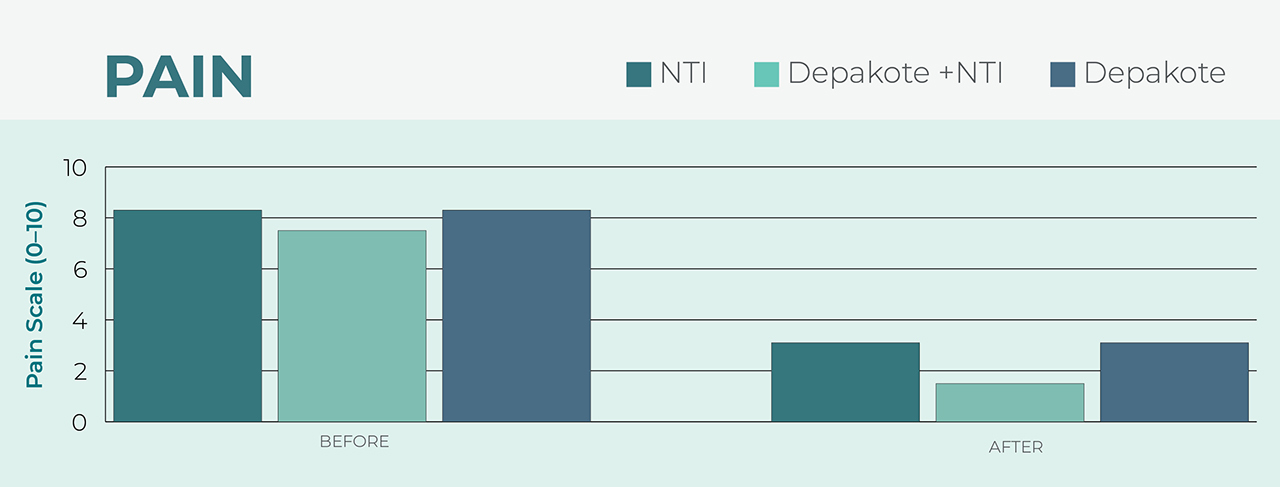
The NTI-tss has also been shown to be as effective as Depakote, a commonly prescribed pharmaceutical migraine preventive medication, without any of Depakote’s side effects. These side effects include weight gain, alopecia, fatigue and liver function abnormalities. Several pharmacological products approved for migraine prevention are associated with adverse side effects, including birth defects. The NTI-tss Plus is a safe and effective alternative.
RC: How is the NTI-tss Plus different from full-arch splints?
JB: With a full-arch splint, all the teeth occlude with the splint, and the patient has a flatter, more efficient surface to clench into. This can allow muscle contraction to intensify. It is only during an excursive movement — when the splint’s anterior guidance or canine rise occurs and posterior teeth are discluded — that a reduction in intensity of joint strain occurs.
By contrast, the NTI-tss Plus provides instant and continual canine and posterior disclusion, reducing clenching intensity by 70%.
RC: How is the NTI-tss Plus different from anterior deprogrammers?
JB: Anterior deprogrammers are designed to be used “in the chair” in the attempt to deprogram lateral pterygoids in a short period of time and should never be used as therapeutic devices during sleep, as they are not designed to anticipate excursive and protrusive mandibular movements.
Additionally, the NTI’s proprietary design eliminates not only posterior contact but also canine contact, further reducing the ability for muscles of mastication to fire.
RC: What did the NTI Patterns of Use Survey show regarding success rates and side effects related to the NTI?
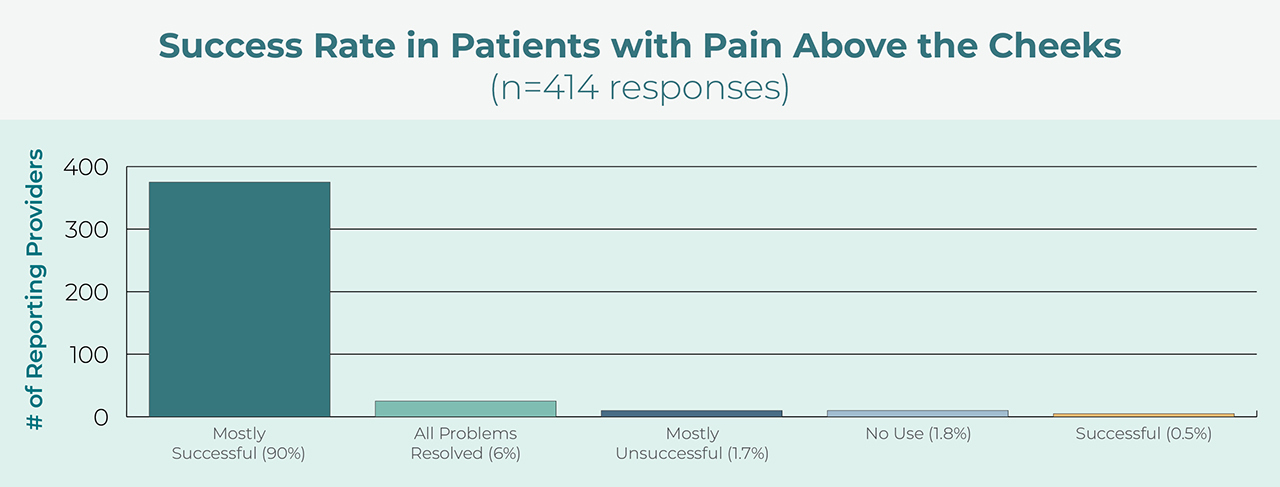
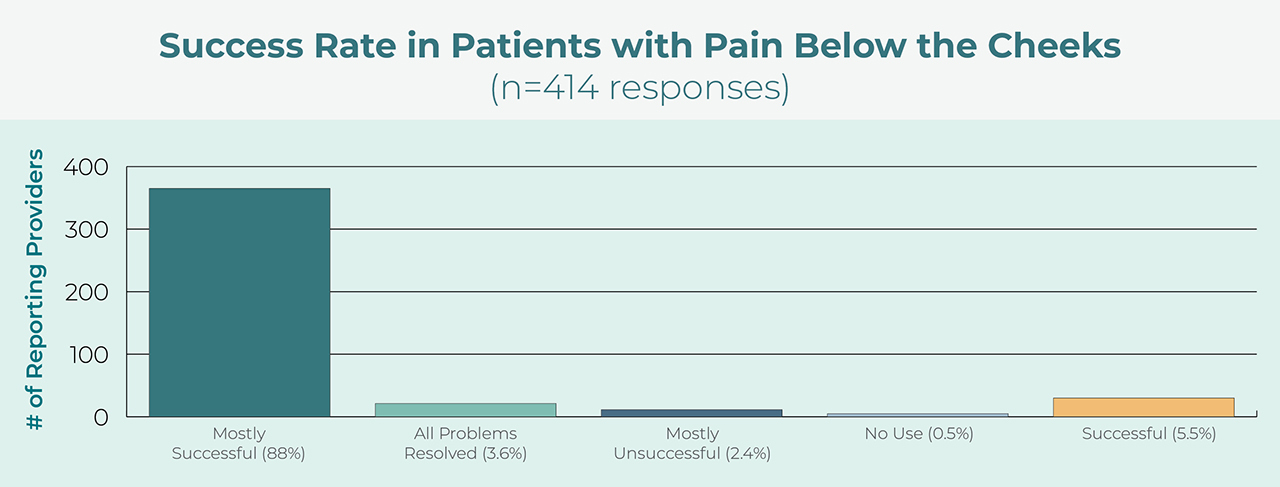
JB: According to a survey of more than 575 dentist respondents responsible for the delivery of over 75,000 NTI cases, the NTI was “mostly or completely successful” in eliminating pain above the cheeks in 96% of cases. The NTI was also “mostly or completely successful” in the elimination of pain below the cheeks in 91.6% of cases.
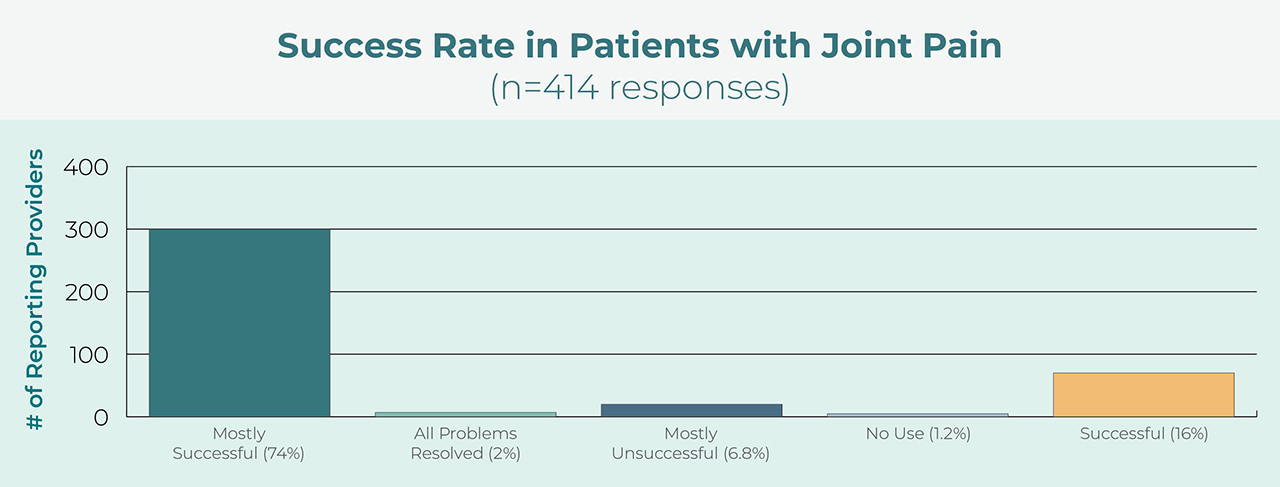
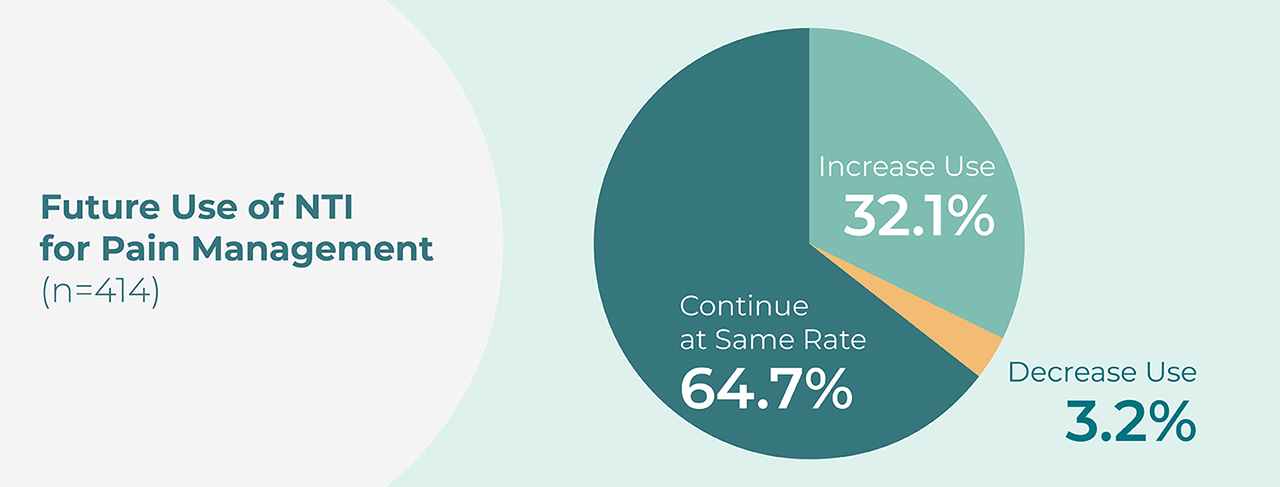
Approximately 65% of the respondents stated that they plan to use the NTI at the same rate, while more than 32% planned to increase their frequency of NTI use.
An undesired occlusal change occurred in only 1.6% of cases. Some misinformed clinicians speculate that these changes are due to supraeruption of posterior teeth or intrusion of anterior teeth. This just isn’t true. What can happen is what we as clinicians always strive for: normalization of the lateral pterygoids, which can allow the condyles to seat more superiorly into centric relation — if they weren’t there already. In some patients, it happens in a profound manner with the mandible pivoting at the palatal cusps, thereby revealing them as true interferences to centric relation, which hadn’t been presented prior to treatment.
Another unfounded concern is that a patient can aspirate their NTI because of its small size. The survey revealed zero instances of aspiration confirmed by radiograph.
To address the concerns of this small percentage of clinicians, we developed the NTI OmniSplint® with the help of the Transform Dental Sleep team. This dual full-arch appliance follows the NTI therapeutic protocol of even contact at the opposing midline, canine and posterior disclusion in centric and all excursions, and minimal vertical dimension of occlusion. This patented protocol and design eliminates any concerns over potential occlusal changes or dislodgement during sleep. The dual arch design also ensures smooth transitions in all excursions.
To learn more about the NTI-tss Plus and the NTI OmniSplint, visit glidewell.com or call 866-335-0744.
Blog Post
Magazine Articles

NTI-tss Plus is a registered trademark of Boyd Research, Inc. NTI OmniSplint is a registered trademark of James Boyd.
Send blog-related questions and suggestions to hello@glidewell.com.

2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.