2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.
800-854-7256 USA
Diabetic patients require screening for sleep apnea.

I have recently seen several journal articles that refer to Type 2 diabetes and obstructive sleep apnea (OSA) as epidemics in America. While there is no direct causal link between the two conditions, they are found together in the same patient population. When a patient self-identifies as prediabetic or diabetic, dental teams naturally are on the lookout for gingivitis, periodontitis and oral candidiasis. Diabetes is very commonly associated with sleep apnea, particularly when the patient is obese. This post will describe diabetes and sleep apnea, as well as the prevalence of these conditions and treatment strategies for patients.
Type 2 diabetes is a nutrition-based chronic condition that is comorbid with high blood pressure, obesity, kidney disease and sleep apnea. The Centers for Disease Control and Prevention (CDC) states: “With Type 2 diabetes, your body doesn’t use insulin well and can’t keep blood sugar at normal levels. About 90–95% of people with diabetes have Type 2. It develops over many years and is usually diagnosed in adults (but more and more in children, teens, and young adults).”
Diabetes
Prediabetes
Obstructive sleep apnea is often associated with snoring. It is important to note that OSA patients often snore, but not all snorers have OSA.
OSA is a seemingly unrelated disorder with very clear symptoms. This type of apnea is characterized as a cessation of breathing for 10 seconds or longer with patient effort, in which the sleeping patient struggles to breathe against an obstruction that occludes the airway. These obstruction events occur when the tissues of the throat relax during sleep and collapse into the airway. They resist increased patient effort, heart rate and blood pressure. Patients often sweat and wake up gasping and choking. Once the patient finally wakes up enough to clear the obstruction and resume breathing again, the heart rate begins to normalize — only to have the cycle start over again once the patient resumes the sleep pattern. This cycle is repeated many times per hour for OSA patients.
The sleep-wake cycle that goes on throughout the night is known as sleep fragmentation. This fragmented sleep cycle results in extreme tiredness, particularly in the afternoon — and it can lead to vehicle accidents, reduced job performance and impacted quality of life.
Patient classifications of sleep apnea are as follows:
Patients with sleep apnea seek treatment primarily for two reasons:
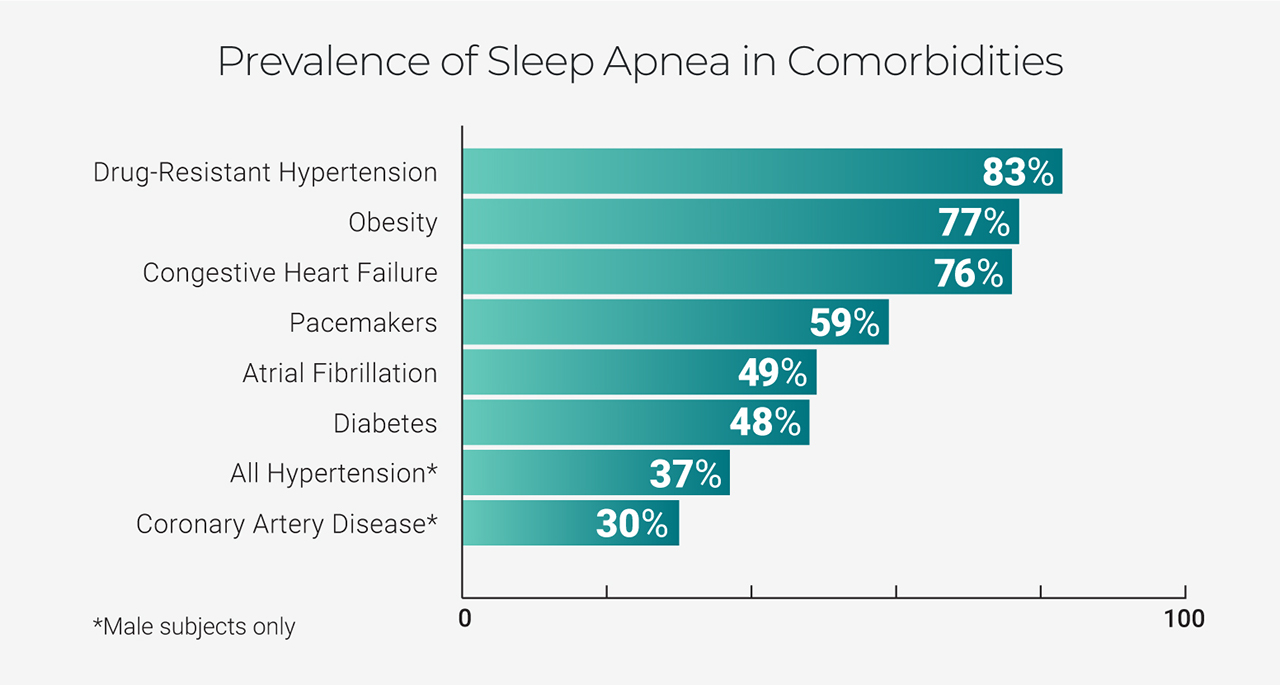
Prevalence of Sleep Apnea
Obstructive sleep apnea is caused by the collapse of the upper airway; the resulting hypoxia and sleep fragmentation causes sympathetic arousals and sleep fragmentation. OSA is estimated to occur in 86% of obese patients with Type 2 diabetes.
OSA is generally associated with a reduction in overall sleep time, which has been found to play a role in altering glucose metabolism. One laboratory study found that exposure to five days of four-hour sleep durations was associated with a 40% reduction in glucose tolerance to intravenous glucose and a 30% reduction in the acute insulin response.
Treatment of OSA and snoring has a measurable impact on the patient’s ability to metabolize glucose. Treatments of OSA include lifestyle and behavioral practices such as establishing good sleep hygiene and weight loss, both of which will have a significant impact on OSA.
Surgery
Surgical procedures for sleep apnea are generally used to reduce the amount of tissue of the oral cavity and upper airway. These procedures include nasal surgery (such as septoplasty or turbinectomy), tongue reduction surgery or genioglossus advancement (move the tongue forward by advancing a small part of the jaw). Other treatments include reducing the tissues of the upper airway. Uvulopalatopharyngoplasty involves trimming the soft palate and uvula and removing the tonsils. Laser-assisted uvuloplasty (LAUP) involves scarring of the soft palate with laser and reducing the uvula. Maxillomandibular osteotomy (MMO) and advancement (MMA) surgeries involve the advancement of the maxilla and the mandible, which makes the airway larger. These are invasive procedures that take some months to fully recover from.
Tracheostomy is an effective surgery for sleep apnea. This surgery involves making a hole in the throat that can be capped during the day for speaking and breathing, but removed at night in order to bypass areas of obstruction and breathe easily. This procedure is typically not the first choice except in very severe cases.
Stanford University studied the issue of surgery for sleep apnea and found that the challenge with surgery for this condition is that patients present with more than one site of obstruction. In its study of 415 patients, only 25% presented with a single site of obstruction. Clearly, single-site surgery would have a poor success rate. By comparison, combinations of surgical interventions to address specific obstructions brought the success rate to around 95%.
Medical Treatment
Continuous positive airway pressure (CPAP) devices are considered the gold standard of therapy for obstructive sleep apnea. CPAP devices sit on the nightstand and blow air at a prescribed pressure into the patient’s airway via a hose and mask. This column of air acts as a pneumatic splint to prevent airway collapse. As with any therapy, the patient needs to wear it in order for it to work.
These devices look invasive, and depending on the pressure setting and the severity of the patient’s sleep debt, success with CPAP requires coaching and patience. Sadly, both of these conditions are often at a premium. A 2015 study showed that after 10 months of use, 48% of OSA patients abandoned CPAP therapy because they disliked CPAP.
Dental Therapy
Mandibular advancement device (MAD) therapy (also referred to as oral appliance therapy) is the dental treatment for sleep-disordered breathing. MADs hold the mandible in an advanced position much like the position that surgeons achieve with MMA surgery. MAD therapy is a nonsurgical therapy that can be adjusted as conditions change over time on the advice of a trained dentist.
The advanced position of the jaw applies tension to the muscles and ligaments of the upper airway, reduces airway collapse, stops snoring, and improves sleep quality and duration. A recent study comparing patient preference between MAD and CPAP found that 74% of the study participants preferred MAD over CPAP.
In summary, the connection between diabetes and OSA is clear: Patients treated for OSA exhibit a positive effect in their Type 2 diabetes. This is particularly true for patients who have been treated with CPAP. The size of these studies is still very small and there is a great deal left to do, especially in the area of mandibular appliance therapy. However, there is at least one study in which mandibular advancement devices were fabricated for patients with OSA and Type 2 diabetes. The appliances were set at 50% of each patient’s range of motion with 20% of maximum interincisal opening. Results were positive, and in this case “a statistically significant difference was seen in all outcomes after intervention with MAD in all groups except Type 2 diabetes levels in participants having severe OSA.”
The ADA has taken a stance on the role of the dentist with regard to both diabetes and sleep-disordered breathing. Updated health history and initial screening with questionnaire are all that are required to confirm that patients with diabetes are screened and treated in the dental office for snoring and OSA.
To learn more about snoring and OSA, as well as receive a straightforward protocol for screening and treating patients, visit glidewelldental.com/pmad or enroll in a free online dental CE course.
Send blog-related questions and suggestions to hello@glidewell.com.

2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.