2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.
800-854-7256 USA
Treatment for sleep-disordered breathing does not have to be limited to diet alone.


Excess body weight is directly linked to sleep-disordered breathing (SDB), a condition in which breathing repeatedly stops and starts during sleep. This occurs when soft tissues of the airway relax during sleep, causing the airway to narrow and become blocked. Snoring is due to a partially collapsed airway, whereas, with obstructive sleep apnea (OSA), the airway is completely collapsed and there is no airflow for 10 seconds or more, in spite of the patient’s efforts to breathe.
When body weight increases, fat tissues can build up in the soft tissues of the airway, resulting in a narrower airway and a higher probability of airway collapse. The two primary symptoms of SDB are snoring and daytime sleepiness, which occurs as a result of the patient waking to breathe many times per hour of sleep.
The three most predictive elements for sleep-disordered breathing are obesity, age and gender. Obesity is a factor because of the fat tissue buildup in the airway and related narrowing. Age is a recognized factor in sleep apnea in cross-sectional and longitudinal studies; however, the mechanisms by which these risk factors increase sleep apnea susceptibility are not known. Data on men and premenopausal women has shown a three- to fourfold greater prevalence of OSA in men, although the prevalence of sleep apnea in postmenopausal women is similar to that of men.
Through data, we gain a clear picture of the obesity epidemic in the United States. The Centers for Disease Control and Prevention (CDC) states: “The age-adjusted prevalence of obesity among U.S. adults was 42.4% in 2017–2018. The prevalence was 40.0% among younger adults aged 20–39, 44.8% among middle-aged adults aged 40–59, and 42.8% among older adults aged 60 and over.” (See Fig. 1.)
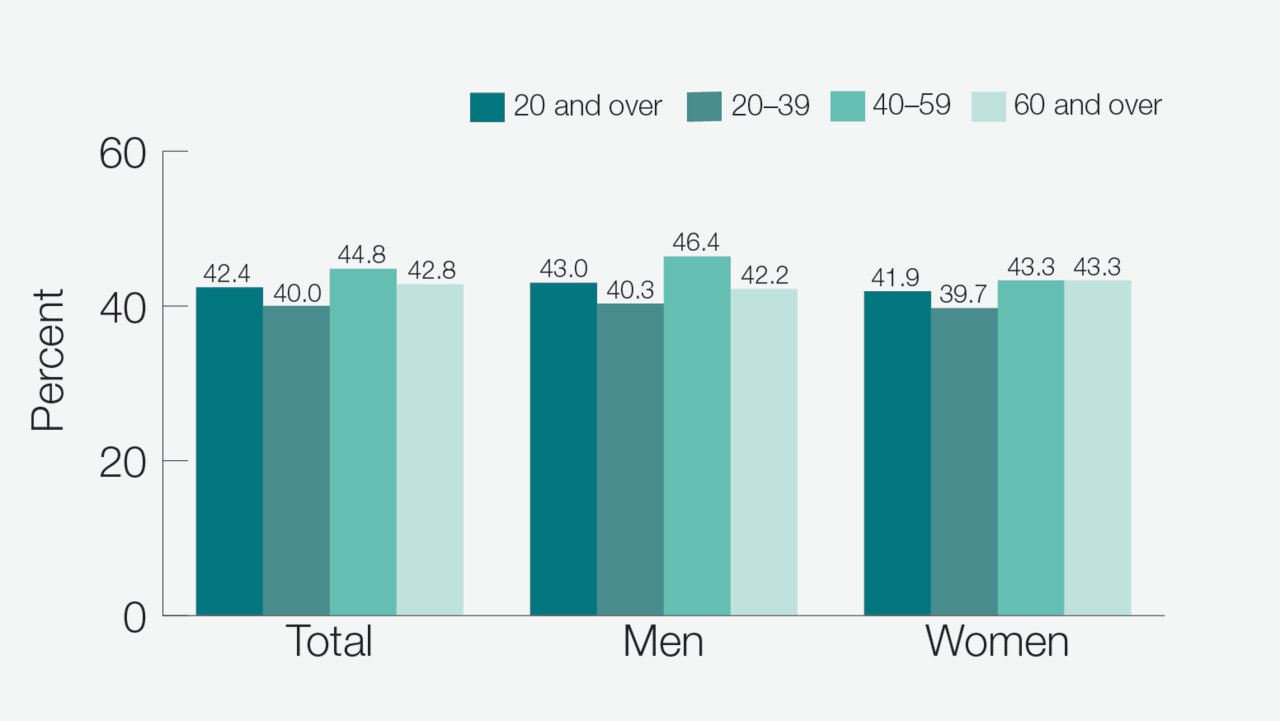
Figure 1: Prevalence of obesity among adults aged 20 and over, by sex and age in the United States, 2017–18.
Source: CDC/National Center for Health Statistics
The University of Wisconsin School of Medicine conducted an investigation of weight change and SDB. This study followed some 948 patients for more than four years. The results were compelling: “Relative to stable weight, a 10% weight gain predicted an approximate 32% (95% confidence interval [CI], 20%–45%) increase in the AHI. A 10% weight loss predicted a 26% (95% CI, 18%–34%) decrease in the AHI. A 10% increase in weight predicted a sixfold (95% CI, 2.2–17.0) increase in the odds of developing moderate-to-severe SDB.”
The authors of this study went so far as to suggest, “Our data indicate that clinical and public health programs that result in even modest weight control are likely to be effective in managing SDB and reducing new occurrence of SDB.”
Primary treatment of mild to moderate SDB should include a discussion about weight loss. However, for many patients, compliance with diet and exercise regimes as a sole treatment for SDB can be challenging, especially considering the sustained effort that is required over time to achieve a 10% change in body weight. For example, a 230-pound man would need to lose 23 pounds. This 10% weight loss would be effective and noninvasive — but very difficult and time-consuming. For adults who have tried dieting at one time or another, their experience is likely to color their confidence in diet alone as a possible solution to SDB.
When lifestyle changes are found to be too difficult or efforts to change do not yield desired results, other therapeutic interventions, such as oral appliance therapy (OAT), should be considered in combination with lifestyle changes, rather than no treatment at all. OAT is the management of airway collapse by wearing a mouthpiece during sleep to hold the jaw in a dentist-prescribed advanced position. This advanced position has been shown to activate the muscles and ligaments of the airway to prevent collapse and obstruction.

To prevent snoring and sleep apnea, patients may consider oral appliance therapy in combination with lifestyle changes. The Silent Nite® Sleep Appliance treats sleep-disordered breathing quickly and effectively.
It is important to realize that OAT is a successful remedy that manages the airway during sleep for a patent airway. This early step can help the patient regain energy and support a healthy, vibrant lifestyle that includes nutritious food choices and exercise, which have the potential for maximizing long-term weight-loss goals.
To learn more about snoring and OSA, as well as receive a straightforward protocol for screening and treating patients, visit glidewelldental.com/pmad.
Send blog-related questions and suggestions to hello@glidewell.com.



2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.