Dental CE
- Free online CE course by Mark E. Abramson, DDS: “Introduction to Dental Sleep Medicine”
Snoring and Sleep Apnea Article
- Randy Clare, Glidewell: “How to Select the Best Anti-Snoring Solution for Your Patient”
800-854-7256 USA
Subheading goes here...



How is it possible that an appliance that was developed in 1909 for treating malocclusions is now dominant in the treatment of snoring and sleep apnea? To understand, we must take a look back at the history of the device as well as the innovations that led to its modern-day use.
In his 2003 paper “History, Background, and Development of the Herbst Appliance,” which cited an unpublished survey of the top six major orthodontic laboratories in the United States, Dr. Hans Pancherz reported the Herbst appliance had grown to be the most popular functional appliance for the treatment of Class II malocclusions.
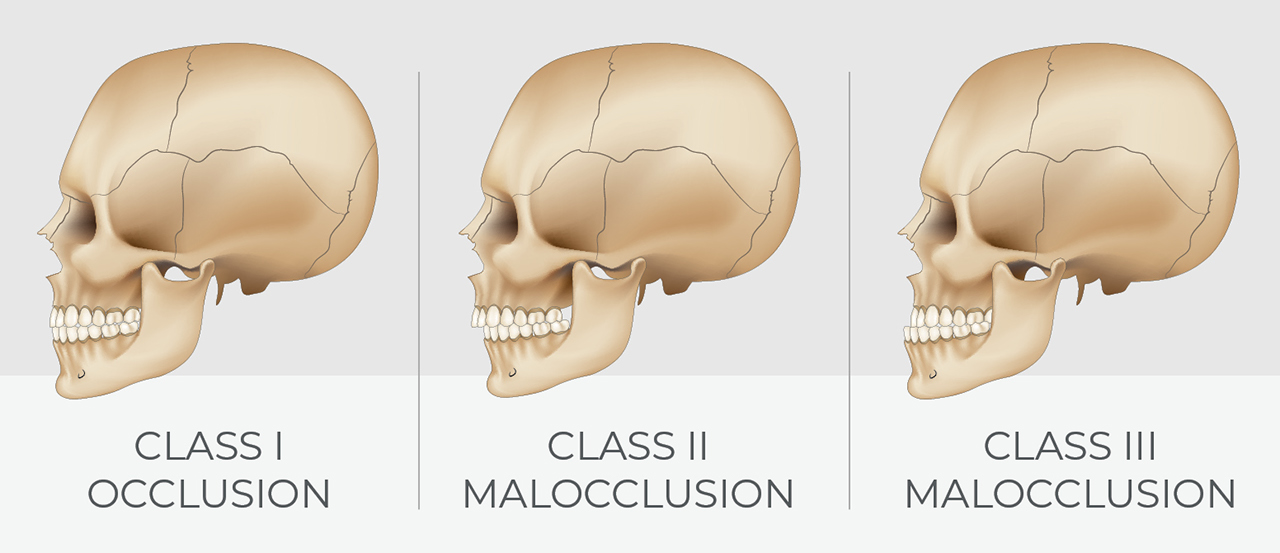
Types of dental occlusions.
Dr. Emil Herbst (1872–1940), who invented his eponymous appliance to correct Class II malocclusion, made many contributions to the field of dentistry; his most famous design appears in the literature in 1909 for the Fifth International Dental Congress in Berlin. To remove patient compliance as an obstacle to treatment, the Herbst appliance was designed as a fixed device that acts as a hinge between the maxilla and the mandible. The hinge was made of silver or gold tubes with corresponding rods that forced the mandible forward, but allowed speech, chewing and swallowing.
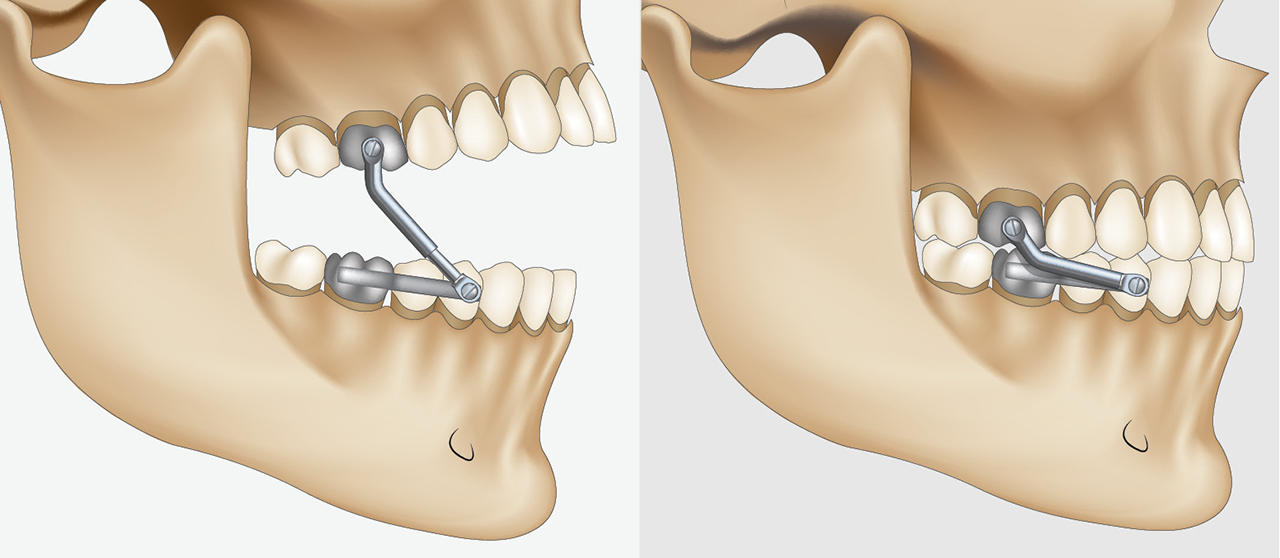
The hinge on the Herbst appliance forces the mandible forward, but allows speech, chewing and swallowing.
Dr. Herbst identified that consistent anterior pressure stimulated mandibular growth. For many years, the length of the rods was fixed, making titration of the device difficult and time consuming. This may have contributed to the appliance falling out of favor with clinicians.
In 1934, Dr. Herbst published a paper on the long-term effects of treating patients with his appliance. Over the next four decades, little attention was paid until Dr. Pancherz revived interest in the Herbst appliance by publishing papers on the appliance beginning in the late 1970s. Since then, he has published 140 scientific articles, 72 of which deal with the Herbst appliance.
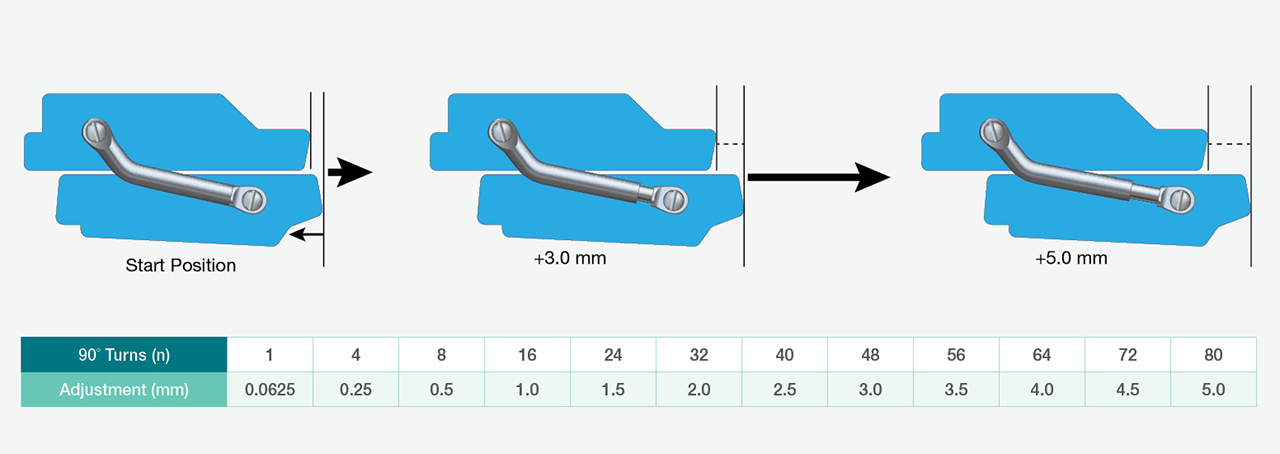
Some Herbst-style appliances, such as the example above, require care for accurate and predicable adjustment due to the limited range of the adjustment screw; 16 turns for 1 mm adjustment per side can be a challenge in a busy dental office.
The device functionality improved with a change to a barrel screw advancement mechanism so that jaw position could be micro-adjusted in increments less than 1 mm, allowing for easier and more precise protrusion. Clinicians commonly report that while barrel screw adjustments are easier than changing the rods, it is easy to lose count of the turns and advance asymmetrically, which is uncomfortable for some patients.
In 1970, Dr. William Dement opened the first sleep diagnostic lab at Stanford University, leading to a boom in sleep apnea diagnoses and patients requiring treatment. Medical doctors from Germany and dentists from the U.S. realized that holding the jaw forward could open the airway in these patients, and soon afterward they began using removable Herbst-style functional appliances for this purpose. The timing of resurged interest in Herbst appliances led by Dr. Pancherz could not have been better.
As the problems of sleep apnea became better known, demand for diagnosis and treatment grew, with dentists increasingly becoming vital members of an airway-centered healthcare team. Inventive, forward-thinking providers and manufacturers have developed dozens of new mechanisms to hold the jaw forward — Dr. Herbst’s hinge remains, but improved.
With more practitioners experienced in treating snoring and sleep apnea in a clinical setting, demands on the appliances have changed. Key to the treatment of the sleeping airway with an oral appliance is finding the correct jaw position — something no available technology provides today.
Research has shown that the effective treatment position varies widely, from almost no protrusion to a maximum-forward posture that patients cannot achieve from their first night of appliance use. Like every adaptive process, progression — from a little to a lot, from inflexible to limber — takes a variable amount of time depending on the patient. Shortcutting the process is more likely to result in abandonment of effort than a quicker route to maximum protrusion. Hence, adjustable mandibular advancement devices are the norm in dental practice. The OASYS Hinge Appliance™, a recent iteration of the Herbst-style design, has a 10-mm range. The dentist specifies a start position; typically, the device can be backed off a millimeter in case even the gently forward original position is more than comfort allows.
No device is perfect, however. There is simply too much human variation in our patient population. Metal-allergic or metal-averse patients may never accept the metal hinge tubes near their cheek tissue.
To treat snoring and sleep apnea, what is required is a jaw position that is advanced enough to maintain an open airway yet comfortable enough for the patient to fall asleep and stay asleep for the whole night. Many patients adapt easily to the Herbst-style device, as it provides maximum room for the tongue and allows the mandible to move freely in all directions except toward the pharyngeal space.
The design of the traditional Herbst appliance has changed a little to accommodate the needs of snoring and sleep apnea patients. However, the basic function of the device has remained the same.
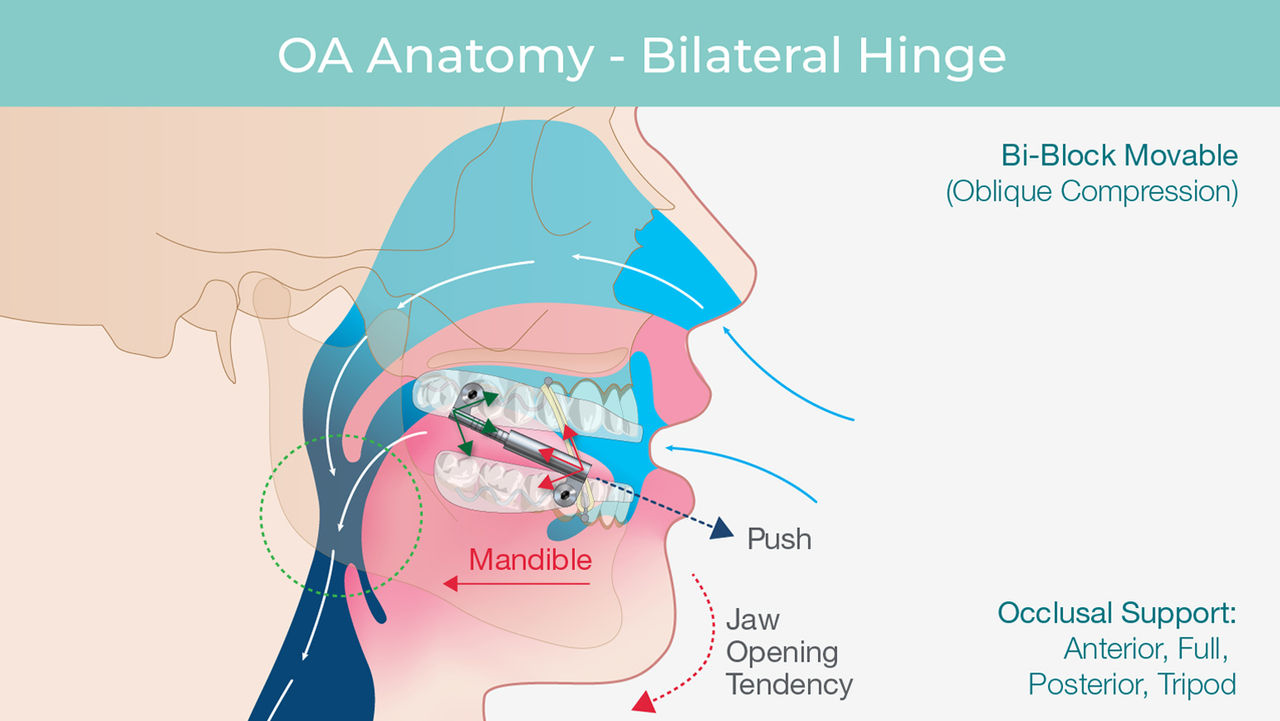
Source: Adapted from Viviano J. OSA appliance anatomy and closing the deal. Slides presented at: Greater New York Dental Meeting. 2019 Dec 4. New York City, New York.
Dr. Mark Abramson from Redwood City, California, was very comfortable with the traditional Herbst appliance, having delivered hundreds to patients in his TMJ and sleep therapy practice. Because many of his patients were covered by Medicare and Medicaid, often struggling with one health compromise or another, Dr. Abramson knew he could increase treatment efficacy by improving the adjustability and ease of use of the Herbst appliance.
Dr. Abramson designed and received FDA 510(k) clearance for the OASYS Hinge Appliance, a Herbst-style mechanism, for the treatment of snoring and sleep apnea. This appliance is also approved for the treatment of patients with Medicare and Medicaid health coverage.

The OASYS Hinge Appliance can be adjusted in or out of the mouth, depending on the clinician’s choice. The scale on the arms of the appliance makes symmetrical advancement easy.
The OASYS Hinge Appliance features a bilateral hinge design that is set in two thermoformed arches that engage the upper and lower teeth. The bite registration is set by the dentist, and the only requirement is a 4 mm interocclusal space for the retention arches. The appliance hinge has no fixed tubes and does not require a pin to be fitted to a barrel screw. A standard hex driver, with an easy-to-hold handle, fits a simple screw mechanism at the front of the appliance. This accessibility allows the appliance to be adjusted while in or out of the patient’s mouth, per the clinician’s preference.
The OASYS Hinge Appliance is micro-adjustable across 10 mm of range. To help keep the adjustments symmetrical, the rods are scored in 1 mm increments to make balanced adjustment intuitive and easy to accomplish. Comparing the length of left and right adjusters is simply a matter of examining the reference points.
The angle of the arms and the fact that this design pushes the jaw into protrusion can encourage an open mouth posture and mouth breathing. Vertical elastics, standard on all OASYS Hinge Appliances, serve to help keep the mouth closed and the lips sealed, encouraging nasal breathing — which is vital to a good night’s sleep.

Notice the score marks on the OASYS Hinge Appliance, which is micro-adjustable across 10 mm of range.
We believe Dr. Herbst would be stunned by the impact that his jaw advancement device has had in the world of sleep dentistry. Oral appliance therapy (OAT) is now recognized as the first line of treatment for snoring and sleep apnea. There have been many rigorous controlled studies that have shown that, while OAT is not as adept in the treatment reduction of AHI (apnea-hypopnea index) as CPAP (continuous positive airway pressure) therapy, OAT patients are much more adherent to therapy than CPAP patients, resulting in better treatment outcomes.
The popularity of the latest generation of Herbst-style appliances like the OASYS Hinge Appliance continues to grow, largely due to Medicare and Medicaid restricting reimbursement to a small number of designs. The Herbst design was the first on this approval list, called PDAC (Pricing, Data Analysis and Coding). As more patients with this coverage are diagnosed, and as more privately funded insurances choose to follow PDAC restrictions, every dentist providing oral appliances to treat snoring and sleep apnea must be familiar with Herbst-style devices.
Thankfully, PDAC does approve other designs with their own unique characteristics, such as TAP® devices (dreamTAP™, TAP 3 TL, TAP) that keep the mouth closed with a different advancement mechanism from that of the Herbst design. To address each patient’s specific clinical needs, the astute clinician must become familiar with several appliance types, material choices, and other features and benefits.
What matters is opening the airway so patients can take every breath easily during sleep. Herbst-style devices, including OASYS Hinge Appliances, are typically easy for patients to accept, and clinicians to deliver and support — and they are approved for reimbursement. This excellent combination allows clinicians to address the community health crisis of sleep-related breathing disorders.
To discover the simple, three-step process to screen and treat patients for snoring and sleep apnea, visit glidewell.com/pmad.
Dental CE
Snoring and Sleep Apnea Article
Send blog-related questions and suggestions to hello@glidewell.com.



2201 Dupont Dr., Irvine, CA 92612
© 2026 Glidewell. All rights reserved.