
In this issue:
Osteotomes: Versatile Instruments in Your Implant Armamentarium
Author


Osteotomes may just be the most versatile instruments in the dental implant armamentarium. These simple instruments can be used in several ways during implant surgery to cut, compress or deform bone to facilitate the placement of implants. They can be used to expand a ridge, condense bone to make it more suitable for implant placement, and “up-fracture” the sinus floor to facilitate a crestal approach sinus lift.
The design of the Hahn™ Tapered Implant Osteotomes (Glidewell Direct; Irvine, Calif.) has further simplified the use of these multifunctional tools in the preparation of implant sites. The Hahn Tapered Implant Osteotome Kit contains a series of instruments that range from 3.0 mm to 5.0 mm in diameter. To ease osteotomy preparation, each osteotome is precisely matched to the contours of the corresponding Hahn Tapered Implant, with laser-etched depth marks that help ensure the length of the implant is not exceeded.
Using an osteotome instead of a rotary instrument to prepare an osteotomy offers some distinct advantages in certain situations. By pushing or laterally condensing bone instead of cutting it away, the osteotome allows the practitioner to predictably place implants in areas where the bone quality or quantity is compromised. The following case examples demonstrate the simplicity with which Hahn Tapered Implant Osteotomes can be utilized in these applications, providing ease of use under challenging clinical circumstances.
CASE NO. 1: BONE EXPANSION AND COMPRESSION
A 63-year-old female presented with an edentulous space in the area of tooth #8 and a hopeless prognosis for teeth #7, #9 and #10 due to advanced periodontal disease (Figs. 1a, 1b). The areas of #8 and #9 were further compromised due to the existence of a nasopalatine cyst. The treatment plan called for the extraction of the untreatable teeth, removal of the cyst, and placement of Hahn Tapered Implants in the #7 and #10 sites to support a 4-unit fixed partial denture. The buccal-lingual width of the ridge below the apices of #7 and #10 was 4.1 mm and 4.2 mm, respectively, indicating the use of osteotomes to expand the ridge and facilitate placement of 3.5 mm implants (Figs. 2a, 2b).
After profound local anesthesia was achieved, teeth #7, #9 and #10 were atraumatically extracted using a small elevator and sharp-beaked forceps (Fig. 3). After thorough debridement of the sockets, a No. 557-L surgical carbide bur was used to perforate the remaining lamina dura of the sockets (Fig. 4). A 1.5 mm twist drill established the proper trajectory for the implants (Fig. 5). The Hahn Tapered Implant Osteotomes were then used in sequential progression (Fig. 6). Taking care to maintain the proper trajectory, the osteotomy was gradually widened, beginning with the 3.0 mm osteotome and finishing with the 3.5-mm-diameter instrument. The osteotomes were driven to full depth with a surgical mallet (Fig. 7). A thumb and index finger were placed on the sides of the ridge to monitor the expansion and confirm that no perforation or labial plate fracture occurred.


Figures 1a, 1b: Anterior and occlusal views of preoperative condition. The prognosis for teeth #7, #9 and #10 was hopeless due to advanced periodontal disease.
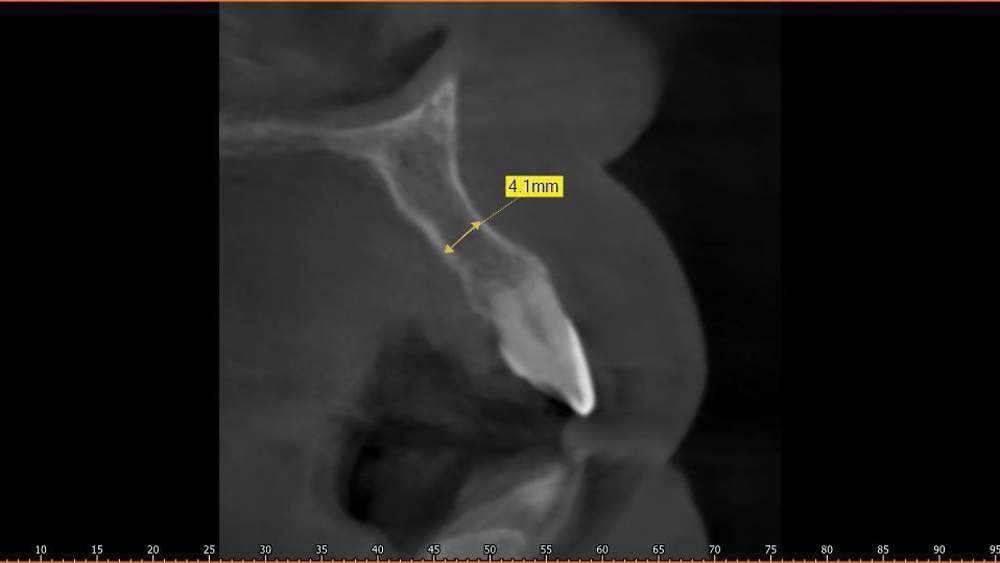
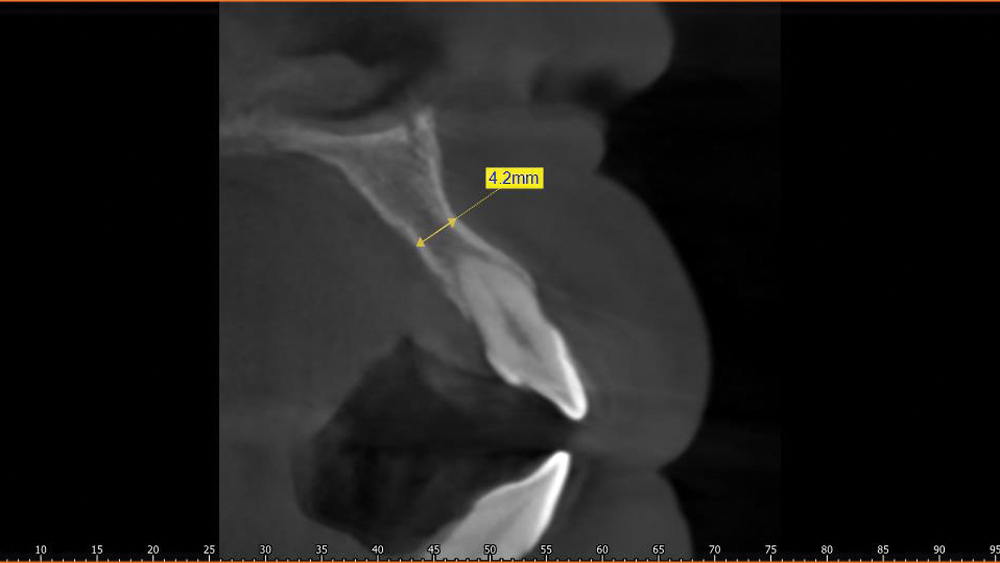
Figures 2a, 2b: CBCT scans illustrate 4.1 mm and 4.2 mm buccal-lingual ridge width in the areas of teeth #7 and #10, necessitating ridge expansion in order to predictably place 3.5 mm implants.
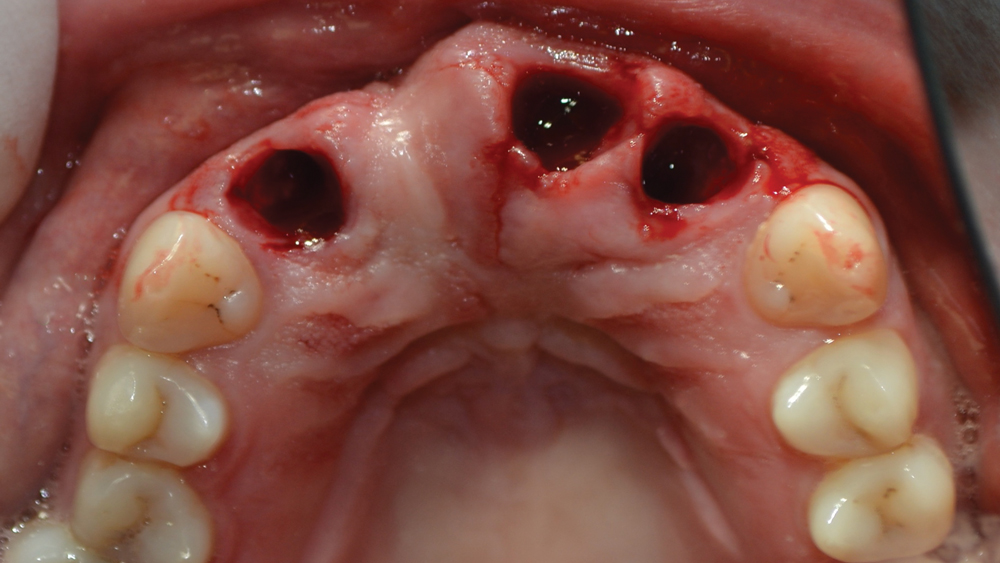
Figure 3: Extraction sites following atraumatic removal of teeth #7, #9 and #10.

Figure 4: The remaining lamina dura was perforated using a No. 557-L surgical carbide bur.
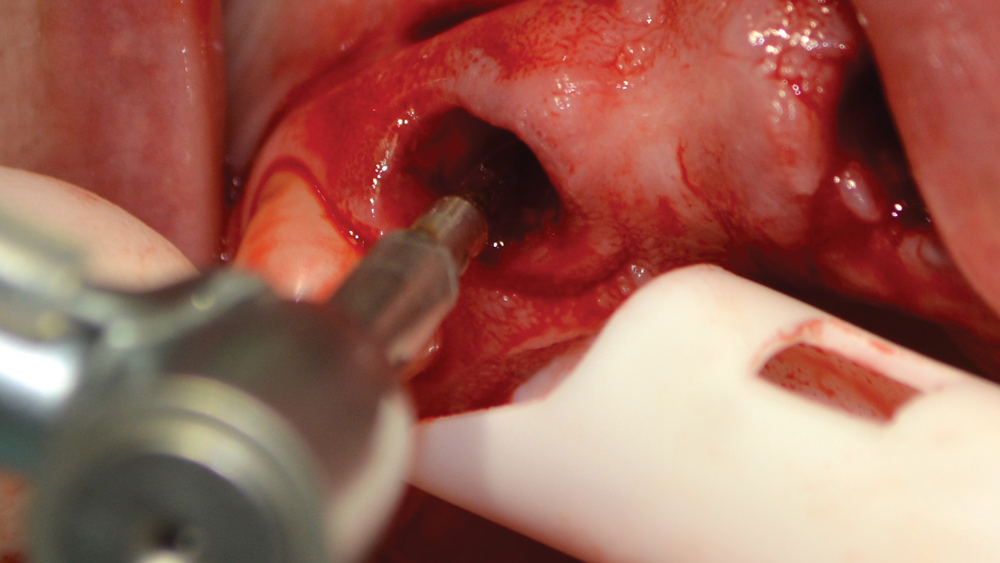
Figure 5: A 1.5 mm twist drill was used to initiate the implant osteotomies at the proper trajectory.
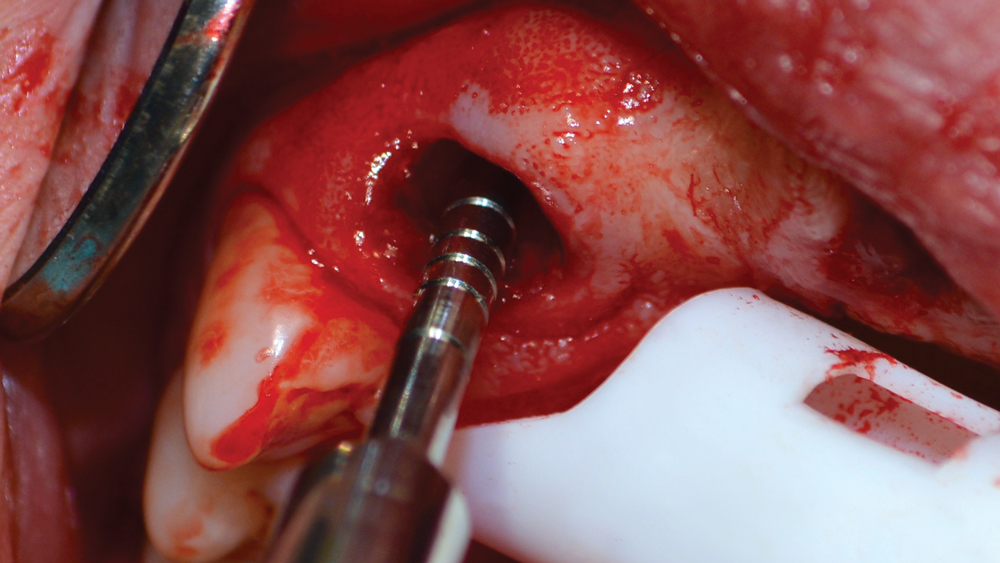
Figure 6: The osteotomy was widened using a series of sequentially larger Hahn Tapered Implant Osteotomes, including the 3.0 mm and 3.5 mm sizes.

Figure 7: The osteotomes were driven to full depth by tapping the end of each instrument with a surgical mallet.
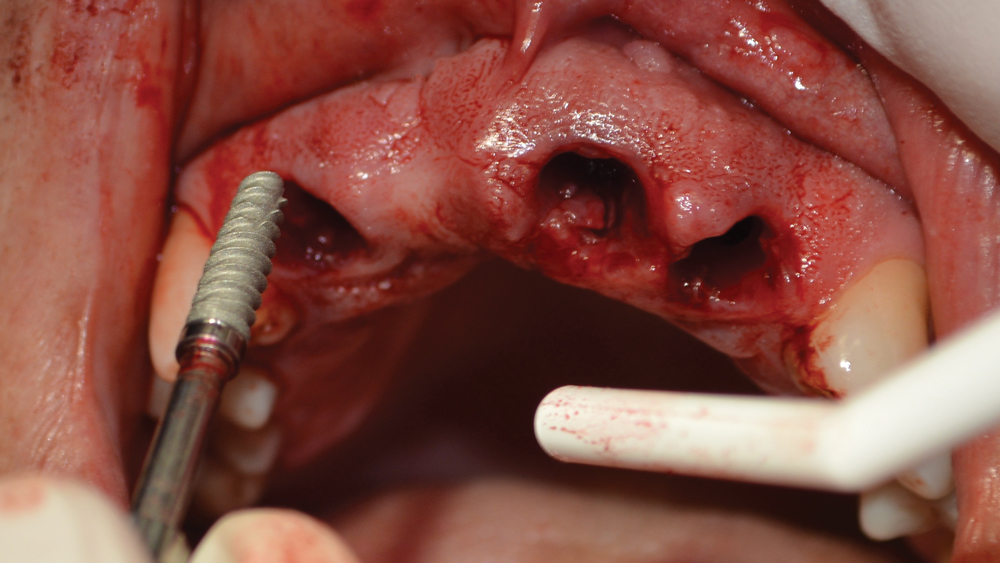
Figure 8: The 3.5 mm x 13 mm Hahn Tapered Implants were hand-tightened into the sites of teeth #7 and #10.
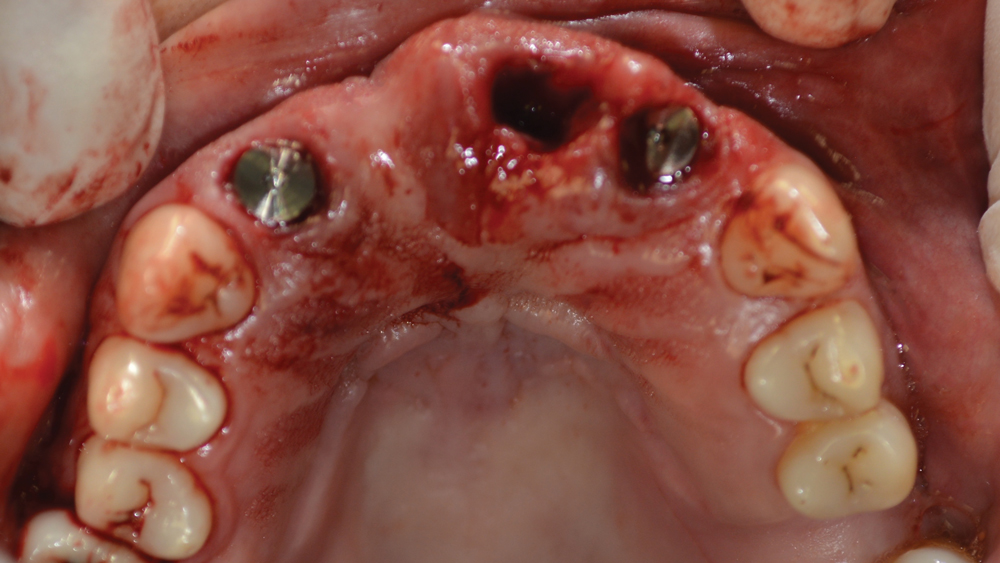
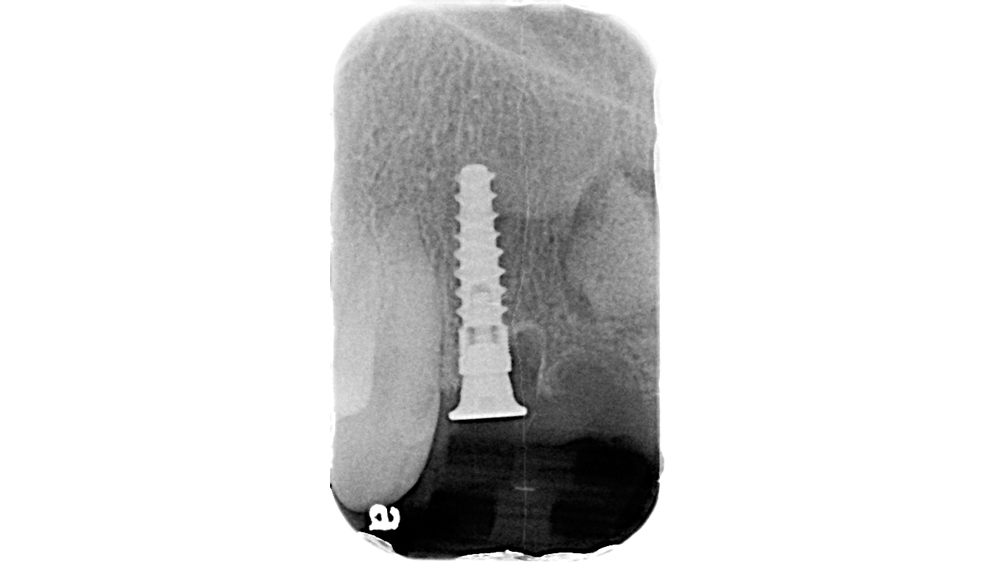
Figures 9a–9c: Healing abutments were placed, and periapical radiographs were taken to confirm complete seating.
Once the osteotomies were completed, a small paddle curette was used to verify continuity of the labial and palatal walls. Two 3.5 mm x 13 mm Hahn Tapered Implants were initially threaded into the sites by hand (Fig. 8). Using a torque wrench, each implant was tightened into final position at 45 Ncm. Then, 3-mm-tall healing abutments were attached to the implants (Figs. 9a–9c). After excising the nasopalatine cyst, the sites were sutured.
When evaluated by the resistance to the initial pilot drill, the bone quality of this patient was assessed as D3 or D4. The use of the osteotome technique for this case not only allowed for expansion of the narrow ridge, but also compacted the medullary bone to help establish excellent primary stability of the implants. Further, the complementary design of the Hahn Tapered Implants and the osteotomes helped facilitate precise, straightforward implant placement, paving the way for a predictable restorative outcome.
The complementary design of the Hahn Tapered Implants and the osteotomes helped facilitate precise, straightforward implant placement.
CASE NO. 2: CRESTAL APPROACH SINUS LIFT
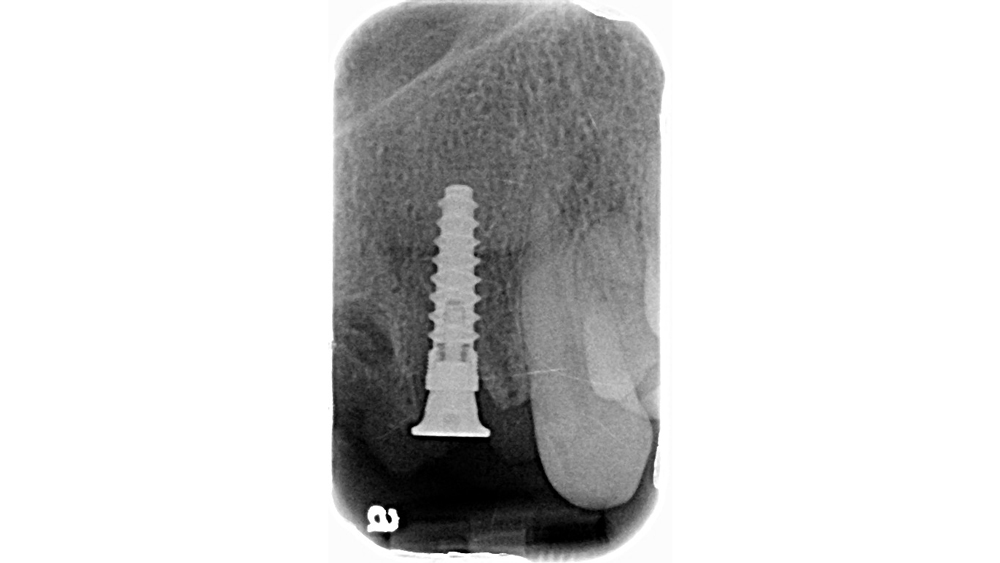
A 64-year-old male patient with an edentulous space in the area of tooth #13 requested implant treatment (Fig. 1). After evaluation of the site, sinus elevation was required to facilitate implant therapy. Preoperative radiography showed approximately 8 mm of bone height available for implant placement (Fig. 2).
After elevation of a full-thickness flap, a 1.5 mm twist drill was taken to a depth of approximately 8 mm and a parallel pin was placed to evaluate the position of the initial osteotomy (Fig. 3). Once the correct trajectory was established, a 3.0 mm and then a 3.5 mm osteotome were used to open the site to the intended implant diameter (Fig. 4).

Figure 1: Preoperative intraoral view of edentulous space in the area of tooth #13, which required a sinus lift to facilitate implant placement.

Figure 2: Preoperative radiography exhibited insufficient space for implantation between the crest of the ridge and the sinus floor.
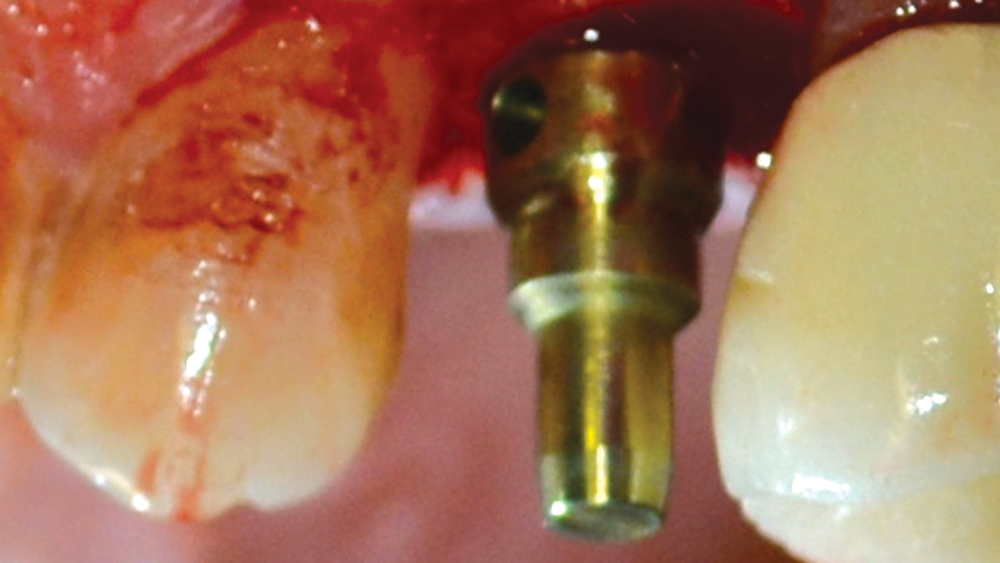
Figure 3: After initiating the osteotomy with a 1.5 mm twist drill, a parallel pin was inserted to evaluate positioning.
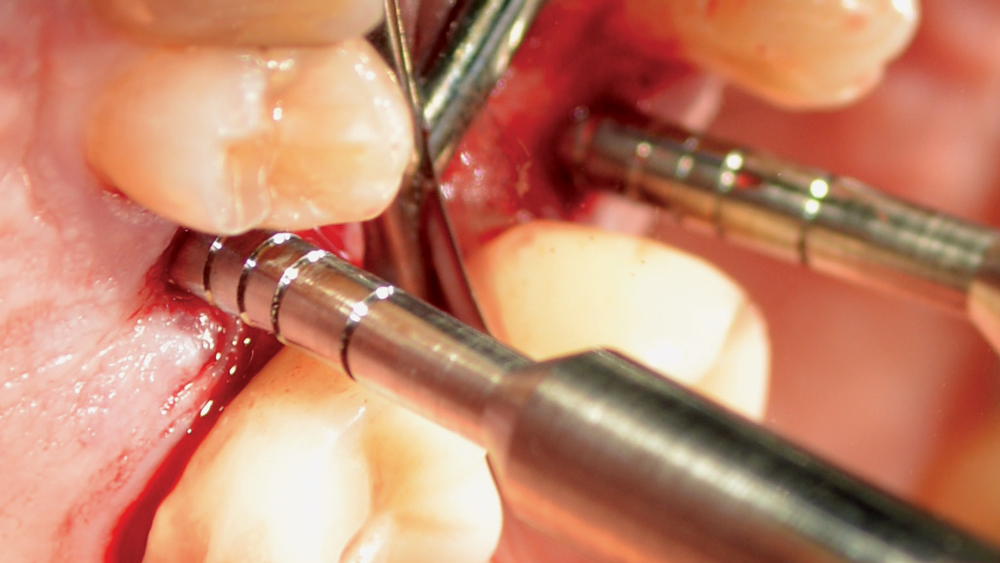
Figure 4: The 3.0 mm and 3.5 mm Hahn Tapered Implant Osteotomes were used to gradually widen the osteotomy.
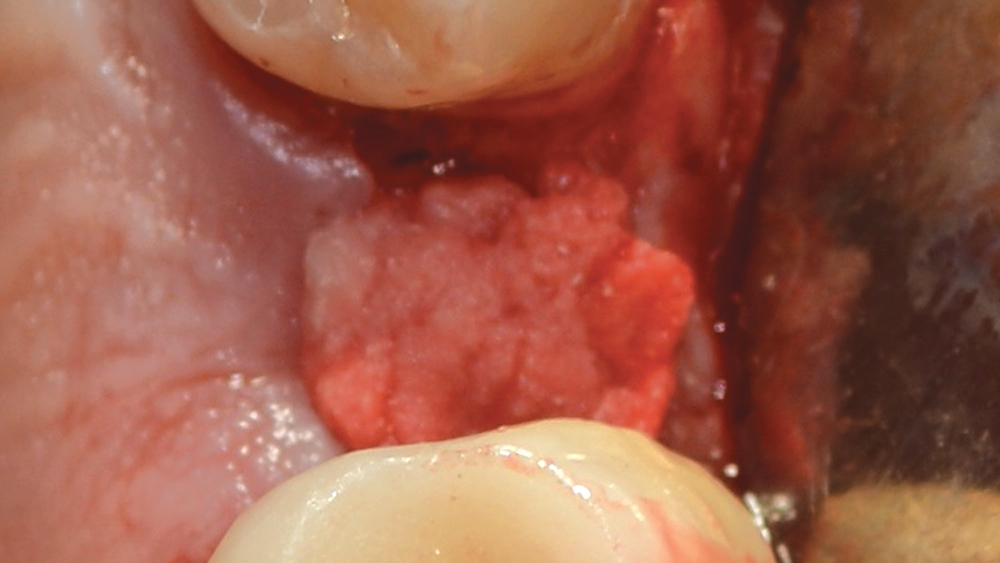

Figures 5a, 5b: Newport Biologics Bone Graft Putty Mineral-Collagen Composite was placed in the osteotomy and pushed into position with a 3.5 mm osteotome.
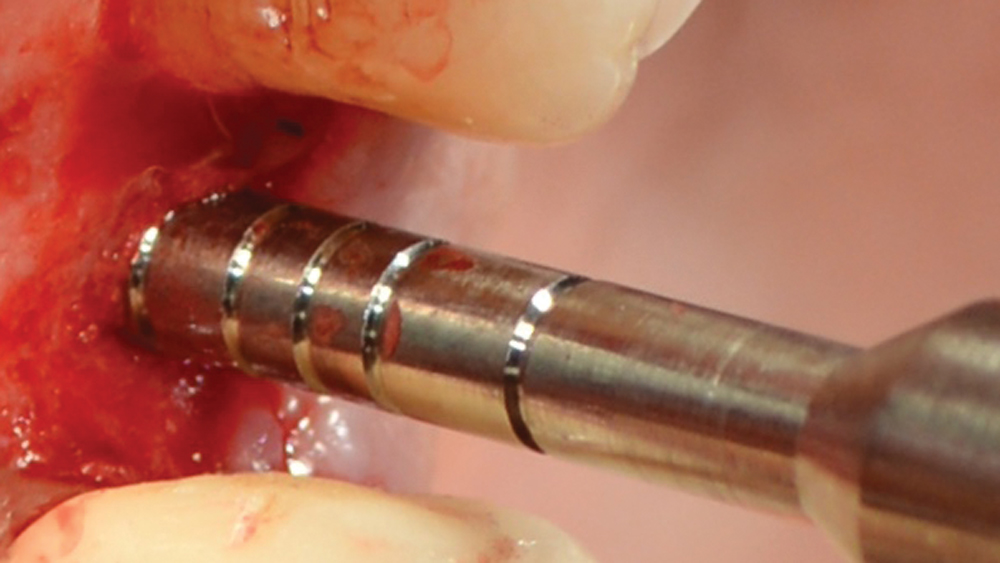
Figure 6: The 3.5 mm osteotome was inserted to a depth of approximately 8 mm and used to up-fracture the sinus floor.
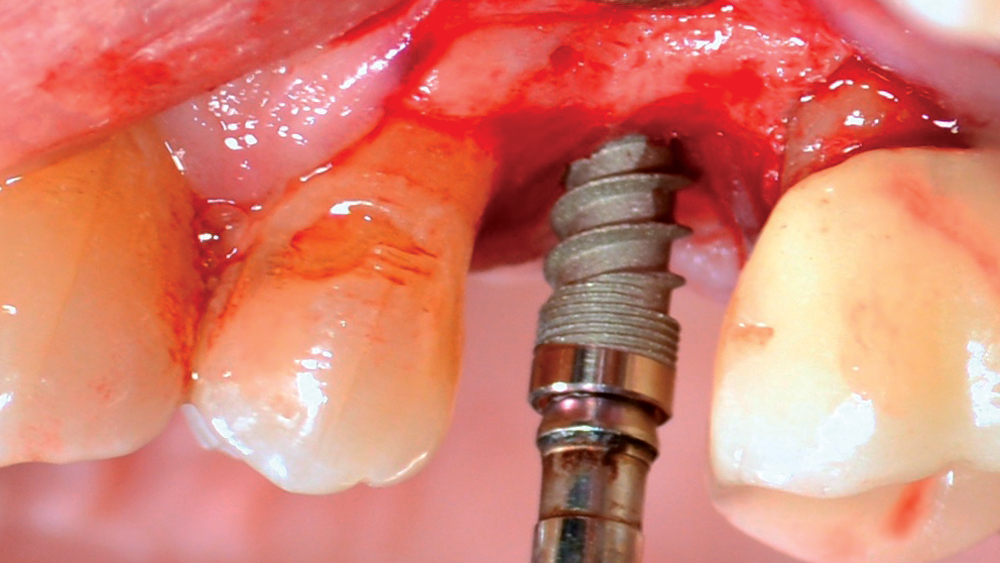
Figure 7: After adding additional grafting material, the Hahn Tapered Implant was placed, completing the elevation of the sinus membrane via hydraulic pressure.
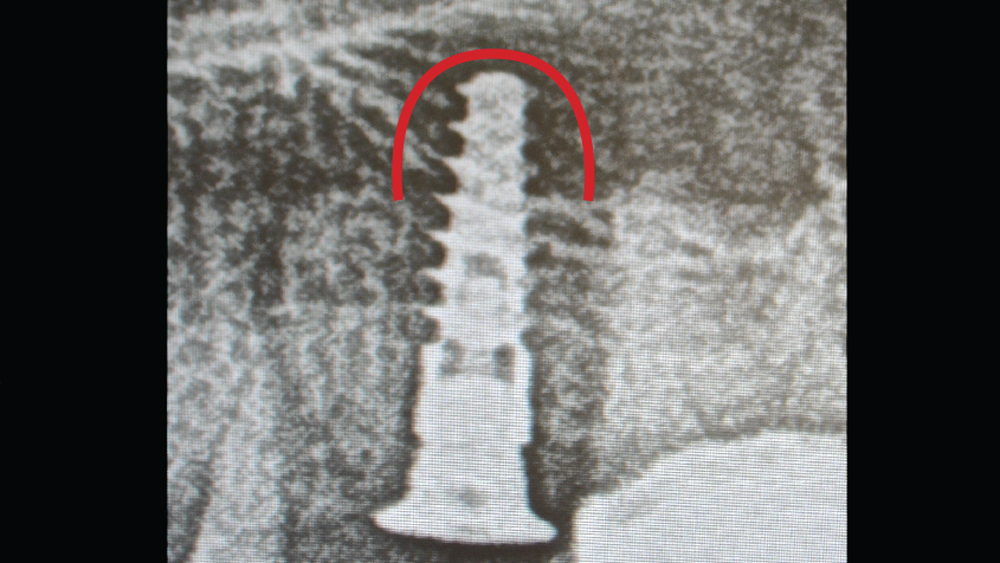
Figure 8: Final radiograph illustrates completed sinus lift via the radiolucent collagen.
Prior to up-fracturing the sinus floor, Newport Biologics™ Bone Graft Putty Mineral-Collagen Composite (Glidewell Direct) was inserted and pushed up using the 3.5 mm osteotome (Figs. 5a, 5b). Once the moldable putty was in proper position, the 3.5 mm osteotome was reinserted and gently tapped to up-fracture the sinus floor (Fig. 6). To check for any perforation, the patient was instructed to commence with a Valsalva maneuver.
Additional grafting material was placed, and a 3.5 mm x 11.5 mm Hahn Tapered Implant was threaded into the prepared osteotomy, completing the uplift of the membrane with hydraulic pressure (Fig. 7). A final torque value of 45 Ncm was achieved. A 3-mm-tall healing abutment was placed, and the soft tissue was repositioned and sutured. The outline of the sinus lift was evident in the final radiograph because of the radiolucent collagen used as the lifting medium (Fig. 8). The collagen will be replaced by native bone after healing, and the Hahn Tapered Implant will serve as a stable foundation for the planned restoration.
CONCLUSION
Osteotomes provide the ability to create more bone volume both in horizontal and vertical directions, making primary stability possible when it may not be attainable otherwise. Engineered to match the precise diameter, length and shape of the selected implant, Hahn Tapered Implant Osteotomes facilitate straightforward site preparation. By adding these versatile instruments to the armamentarium, clinicians can provide efficient, predictable treatment for patients who present with deficient bone quality or quantity.
Osteotomes provide the ability to create more bone volume both in horizontal and vertical directions, making primary stability possible when it may not be attainable otherwise.