In this issue:
My First Glidewell HT™ Implant with Philip Gordon, DDS

Note: The Hahn Tapered Implant System is now known as the Glidewell HT Implant System
Dr. Philip Gordon is a general dentist with a tremendous passion for implant dentistry. Through his popular podcast, “Dental Implant Practices,” Dr. Gordon interviews leaders in the field of implantology and shares tips on the latest continuing education, implant products and practice management strategies for general dentists. Here, he shares what inspired his dedication to dental implants, his reasons for adopting the Hahn™ Tapered Implant System (Glidewell Direct; Irvine, Calif.) and some essential advice for clinicians interested in making implant placement a part of their general practice.
Chairside® magazine: Thanks for being with us today, Dr. Gordon. Can you start off by telling us a little bit about yourself and your involvement with implant dentistry?
Dr. Phillip Gordon: I’m a general dentist in the metropolitan area of Kansas City, Missouri, and implant dentistry is my passion. I’ve really focused on developing the implant component of my general dental practice, and the Hahn Tapered Implant System has been a big part of that. In my podcast called, “Dental Implant Practices,” I interview leading dental implant practitioners from around the world, and I also deliver content on my Facebook group and mentoring page. I try to provide relevant, up-to-date content for general dentists who are placing or are interested in learning to place implants for the benefit of their patients and practices.
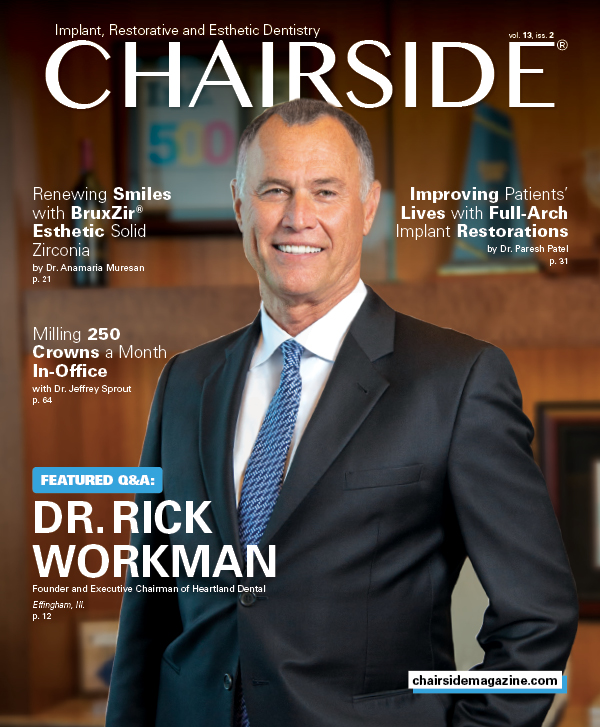
Figures 1a, 1b: Dr. Philip Gordon’s first Hahn Tapered Implant case, a maxillary premolar required extraction due to fracture. Four months later, an implant was placed into the healed extraction site.
CM: In your podcast, you’ve talked about how your background as a general dentist didn’t provide you with much knowledge about implant dentistry. Can you expand on that a bit? Is it due to dental school curriculum or is there more to it than that?
PG: Dental school prepares you well for services like crowns, fillings, partials, dentures — maybe basic extractions and things like that. But they don’t have time to expand upon the intricacies of bone grafting, site development for implant treatment, surgical placement of the implant, or even advanced-level restorations on implants. Those are typically reserved for graduate-level or specialty programs. If dentists want to provide comprehensive implant therapy in their office, there’s a gap they need to jump. I’m trying to break through the barriers and provide dentists with a pathway for CE, essential implant products, and the business side of introducing dental implants in the general dental office.
I’m trying to break through the barriers and provide dentists with a pathway for CE, essential implant products, and the business side of introducing dental implants in the general dental office.
CM: That’s a great service you provide, and something we certainly support in our mission at Glidewell Dental. As someone who helps direct dentists to the resources and continuing education they need to make implant therapy part of their practice, can you tell us how you learned to place implants yourself?
PG: I learned to place implants through a lot of hands-on mentorship. I also found institutions that support training for general dentists, partnered up with some great labs and discovered good implant products that were accessible to the GP. I was just trying everything I could to get all the resources, education and training I needed to provide that care.
Now my mission is to streamline that process and deliver the necessary education and resources to other general dentists in a quicker, more direct pathway so they don’t have to do so much searching.
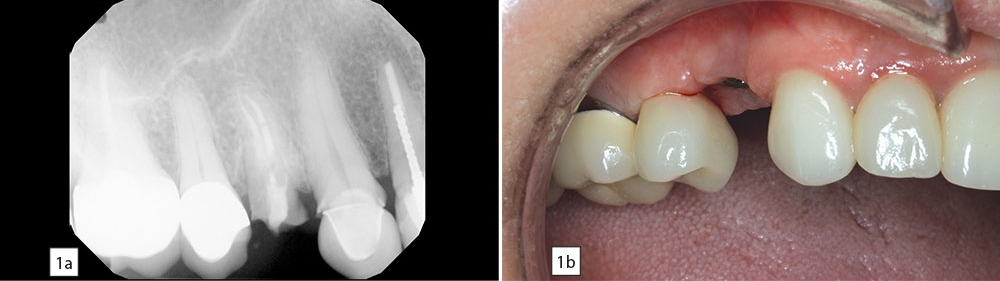
Figures 2a, 2b: Following integration of the implant, a screw-retained crown was delivered, with excellent tissue preservation in the area of the restoration.
CM: Were you restoring many implant cases before you delved into the surgical aspect?
PG: I wasn’t restoring as many dental implants as I would have liked because of the breakdown between treatment planning, communication with various specialists, the multiple visits and the high cost. So I decided that if I could streamline that process with the patients and offer those services in-house, I would be able to not only place some implants myself, but also restore more implants, control the costs, and provide that full-circle restorative care that I think a lot of patients need and desire nowadays.
CM: I noticed that you had Dr. Jack Hahn on your podcast late last year. Can you share your thoughts on the Hahn Tapered Implant System?
PG: I interviewed Dr. Jack Hahn last year and shortly thereafter I flew out and spent a day with him at his office. That was a wonderful experience. He’s a fantastic clinician and a great person. He loves to teach and is so devoted to implant dentistry. Obviously, he’s got the pedigree to back up just an amazing body of work in his lifetime. So I wanted to learn from someone who has been a true pioneer in this field.
As for the implant, it has become the system of choice in my practice for a number of reasons. First, I started using the implant because of Dr. Hahn. I used to prefer the Replace® Select implant, which was a system that he developed with Steri-Oss and Nobel Biocare. So when I realized that he had developed a better implant, I wanted to check that out. After giving the Hahn implant system a try, I really appreciated the aggressive threads for immediate loading, the collar height that allows for predictable healing and the prosthetic adaptability on top. As soon as I learned about the implant and how it was developed by Dr. Jack Hahn, I started switching over to that and have had great success since then. It’s just fantastic that the greatest implant he has designed is named after himself.
I used to prefer the Replace® Select implant, which was a system that he developed with Steri-Oss and Nobel Biocare. So when I realized that he had developed a better implant, I wanted to check that out.
CM: Could you describe your first experience placing a Hahn Tapered Implant?
PG: It was about two years ago for a patient who needed to replace a maxillary first bicuspid. This patient had a failing root canal and was not willing to cut down a canine and another premolar to have a bridge placed. So this was an ideal site for an implant. It’s actually a good area for beginners to place implants because you’re out of the zone of the maxillary sinus and you’re not near any major nerves. I extracted the tooth, did a site preservation graft, came back four months later and placed the Hahn implant. Four months after that, we came back and restored the implant with a screw-retained crown, and the patient is doing great. This was a soft bone area, and the aggressive threads allowed me to get great primary stability.
During that first experience, I found that the surgical kit, the drilling protocol and the integration of the Hahn implant system were quite ideal. It’s very streamlined and straightforward in that you have a specific final drill for each implant diameter and length, and you just work your way up to the size that you need. I appreciate the design of the kit as well as the ease of use because I think it’s important to keep things simple during implant surgery. You don’t want too many components involved, which can overwhelm people. So the kit is laid out very nicely. And the Hahn implant is certainly offered at a user-friendly price point, so we can keep the cost down for the patient, which can help with case acceptance.

In Dr. Gordon’s podcast, “Dental Implant Practices,” he interviews leading implantologists and shares resources and advice for dental implant-minded general dentists.
CM: Can you talk a bit about how implant dentistry has affected the business side of your practice?
PG: Implantology is my favorite part of the practice. It’s also the most profitable part of the practice. Further, it gets the team excited and helps us continue to grow the practice in a way where we don’t have to bring in new patients or do more marketing — we can just operate more profitably with the patient base we already have.
CM: As general dentists make implant placement a bigger part of their practice, how do you see the role of the specialist in all of that? Are there certain cases you refer out and certain ones you keep in-house?
PG: There will be cases where doctors get into implantology and decide that they just love the simple single-tooth cases in the predictable areas of the mouth. The minimal amount of time it takes to do those cases makes them very profitable, and doing that kind of dentistry can be really enjoyable. For the more complex cases, they may want to refer implant placement out and then take care of the restoration, which is also quite rewarding just to see how you can improve the quality of life for patients with severe dental problems.
And then there are GPs who receive advanced training, love what they’re doing, and can do most of the implants in their office. There will still be extreme cases of limited bone or compromised cases where multiple therapies or the team approach is necessary. So it breaks down to each practice, where people are at in their career, and where their desires lie.

Dr. Gordon and a patient discuss implant treatment, which he has made a key component of the comprehensive restorative services offered by his practice.
CM: What tips can you offer general dentists who have decided they would like to learn to place implants?
PG: It’s really important to find a good team. You need to have good team members in your staff. You need to have a good lab to work with for support. You need to find an implant company that supports the general dentist, supports your education, and supports what you’re doing — be that Glidewell Dental or another company — for all those endeavors.
You need to find an implant company that supports the general dentist, supports your education, and supports what you’re doing — be that Glidewell Dental or another company.
I think someone getting into implantology should start slowly. After taking some courses, start with single-tooth replacement and work your way up to multiple-tooth cases. And then it might be an evolution into overdentures. Then maybe eventually it’s fixed full-arch zirconia restorations. But it’s a pathway. You have to get the clinical piece implemented, and you have to get the business side implemented. You have to build your partners while you’re building your education and your clinical skills, keeping that all within your limits of comfort. Along the way you’ll be growing your practice while performing a valuable service that provides the best possible outcome for your patients.