In this issue:
Screw- or Cement-Retained Implant Restoration — or Both?
Author


When placing and restoring implants, one of the most important decisions is whether to provide a screw- or cement-retained restoration. While dentists increasingly prefer screw retention as a means of simplifying crown delivery and avoiding problems related to residual cement at implant sites, both solutions offer distinct advantages and warrant consideration based on the clinical circumstances of each case.1,2,3
CEMENT-RETAINED RESTORATIONS
The primary benefit of cementable implant crowns is that they can be delivered over a custom abutment to correct for implant angulation. In situations that call for a cementable restoration, custom abutments are also beneficial because the margin of the abutment can be carefully positioned by the lab so that it resides at or just slightly below the gingival surface, easing the removal of excess cement. Further, custom abutments are designed to create the ideal “prep” needed for passive seating, a natural emergence profile, optimal crown retention and improved direction of loading forces. Another potential benefit of cementable crowns is the ideal occlusal anatomy resulting from the lack of a screw access hole in the middle of the occlusal table.
The primary disadvantage of cementable restorations is the potential for complications resulting from residual cement at the implant site, which, as mentioned above, can be minimized through the use of custom abutments. Another drawback is the difficulty of removing a cementable crown if access to the implant site is needed for prosthetic maintenance, especially if a permanent cement has been used. One other key consideration is that more interocclusal space is required to achieve the retentive abutment form and height needed for a cementable restoration.
Advantages of Cementable Crowns with Custom Abutments
- Angle correction allows for more flexibility in implant positioning
- Easier to create a passive fit
- Ideal occlusal anatomy due to no screw-access hole
Disadvantages
- Potential for complications from retained cement
- More interocclusal space is required
SCREW-RETAINED RESTORATIONS
If the implant is placed in an ideal position, screw-retained restorations are optimal because they avoid the risk of residual cement impacting the patient’s hard- or soft-tissue health, and they can be removed with relative ease if needed. In the anterior, positioning is ideal when the access channel of the implant restoration exits through the cingulum. In the posterior, screw retention is appropriate when the access hole emerges through the central groove of the crown. One esthetic advantage offered by screw-retained crowns is that the margin of the titanium base of the restoration is situated well beneath the gingival surface, minimizing metal show-through in cases of thin gingival biotype. Screw-retained restorations are also ideal in cases of limited interocclusal space because less restorative space is required.
One possible downside is that the screw access hole causes esthetic concerns for certain patients, which leads some clinicians to opt for cementable restorations when treating the mandible. There is also the potential for the access hole to compromise the location of occlusal contacts. That said, proper material selection can help seal the access hole in a way that seamlessly blends with the surrounding tooth.
Advantages of Screw-Retained Restorations
- Avoid problems with residual cement
- Simple, efficient crown delivery
- Metal-ceramic transition can be subgingvally deeper
- Less interocclusal space is needed
- Ease of restoration retrieval
Disadvantages
- Best used when implant position is optimal
- Access hole can potentially compromise esthetics and occlusal function
A “SCREWMENTABLE” SOLUTION
Now that we’ve explored the pros and cons of screw-retained and cementable implant restorations, let’s take a look at a unique clinical situation where the best solution is a hybrid of the two. With a “screwmentable” solution, a custom abutment is designed to support a cementable restoration, but the crown is created with a screw access hole. The cementation portion of restoration delivery — as well as cleanup of any excess cement — is performed outside of the patient’s mouth. This creates what is essentially a one-piece restoration that avoids any concerns regarding retained cement at the implant site, with greater control over the design of the emergence profile.
CASE REPORT
A patient presented with issues concerning a screw-retained crown in the area of tooth #15. She complained that the crown felt loose, was causing food entrapment and was difficult to clean. Upon examination, it appeared that the prosthetic screw was loose and the restoration was mobile. Removal of the crown confirmed that the current design of the prosthesis created a food trap and was not conducive to soft-tissue health. We agreed that the restoration needed to be replaced. A screwmentable restoration was the optimal solution because the malposition of the implant could be corrected by a custom abutment, thereby minimizing the cantilever. We wanted to improve the direction of loading and lessen sheer forces on the implant site by building the restoration out with the titanium structure of the custom abutment. At the same time, because the implant site was in a hard-to-reach area from which cement removal would have been difficult, screw retention was preferred.
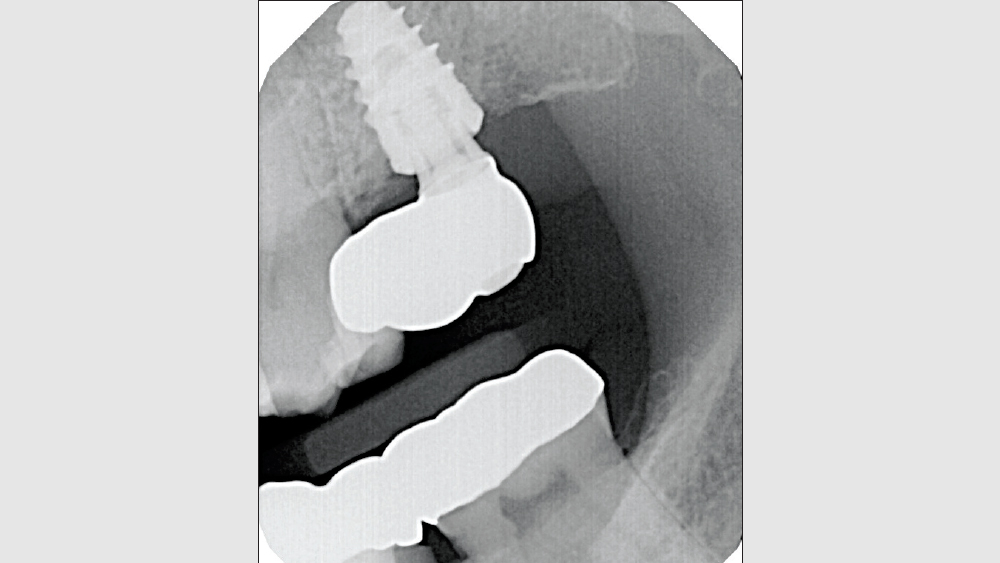
Figure 1: The patient presented with an existing screw-retained crown and chief complaints that the restoration was trapping food and felt unstable. The implant was placed in a nonideal position, and it appeared that as a result, the original restoration was designed with a substantial mesial cantilever.

Figures 2a, 2b: The restoration was removed and screw-loosening was observed. Note the considerable distance between the implant platform and adjacent tooth. Screw retention was not an ideal choice for this patient because this type of restoration required a large material cantilever that resulted in unfavorable distribution of sheer forces at the implant site, food entrapment and screw-loosening. By replacing the restoration with a custom abutment and cementable crown, we could build out the substructure with a titanium custom abutment and correct the angulation of the implant, thereby minimizing the material cantilever.
Figures 2a, 2b: The restoration was removed and screw-loosening was observed. Note the considerable distance between the implant platform and adjacent tooth. Screw retention was not an ideal choice for this patient because this type of restoration required a large material cantilever that resulted in unfavorable distribution of sheer forces at the implant site, food entrapment and screw-loosening. By replacing the restoration with a custom abutment and cementable crown, we could build out the substructure with a titanium custom abutment and correct the angulation of the implant, thereby minimizing the material cantilever.
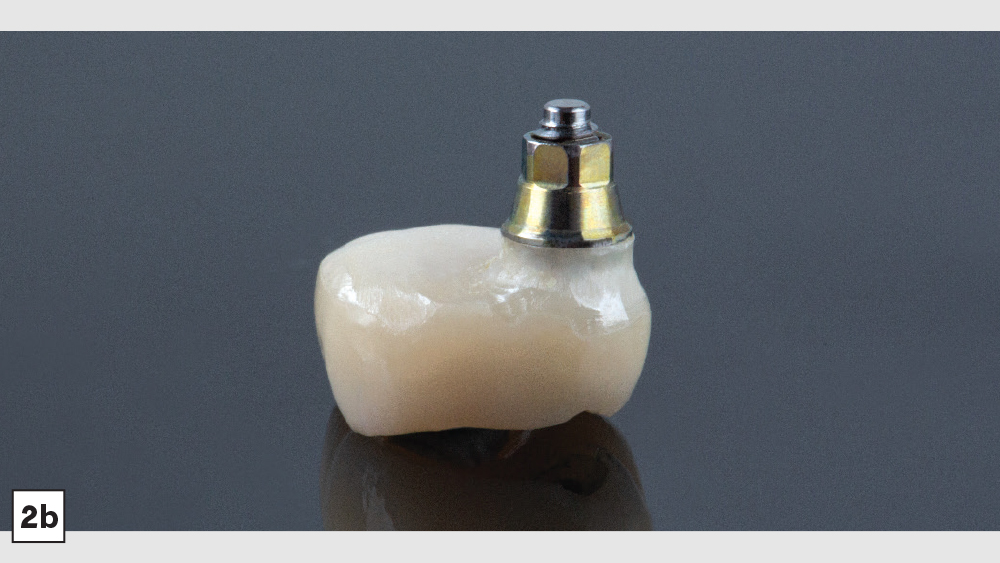
Figure 3: A closed-tray impression was taken and sent to the lab. A model was created from the impression and scanned for CAD design of the restoration. Note the distal angulation of the implant platform, which contributed to the restorative challenges of this case. We requested equigingival custom abutment margins, and selected BruxZir® Full-Strength Solid Zirconia for its ideal strength characteristics. We chose a screwmentable configuration for the restoration because delivering a cementable crown so far back in the mouth would have made removal of excess cement a challenge. Instead, cementation is performed outside of the mouth, with the crown delivered in the manner of a screw-retained restoration.
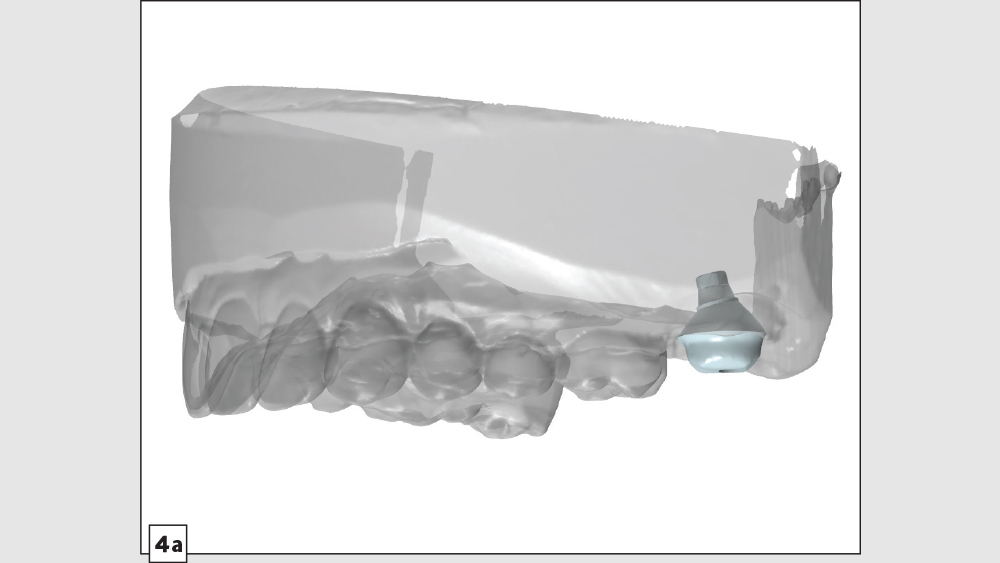
Figures 4a–4c: The custom abutment was digitally designed with an ideal emergence profile, correcting for the nonideal position of the implant while replacing the restorative material cantilever of the prior restoration with titanium contoured to minimize shear forces. The crown was designed with a narrow occlusal table and minimal cuspal heights to direct implant loading down the long axis of the implant.
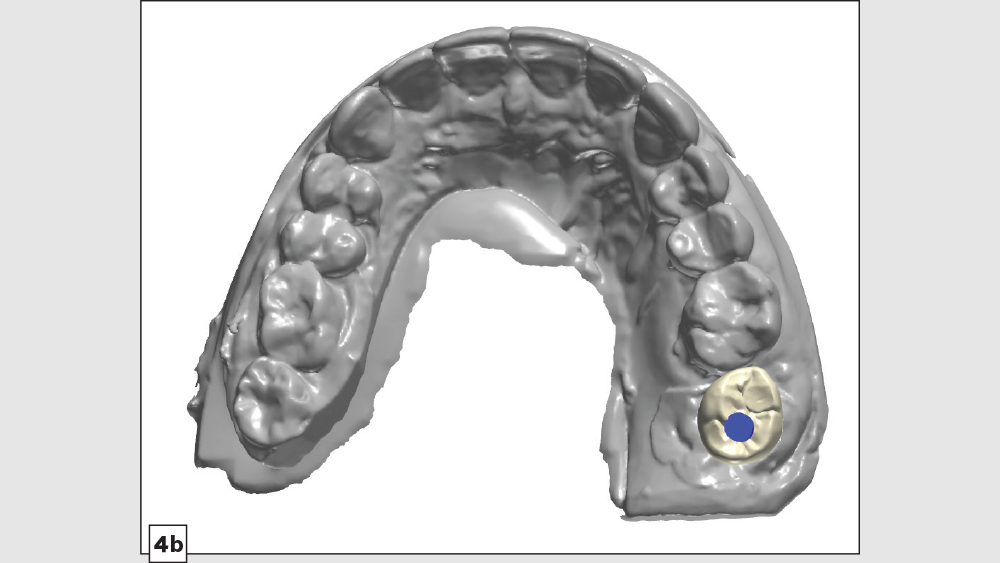
Figures 4a–4c: The custom abutment was digitally designed with an ideal emergence profile, correcting for the nonideal position of the implant while replacing the restorative material cantilever of the prior restoration with titanium contoured to minimize shear forces. The crown was designed with a narrow occlusal table and minimal cuspal heights to direct implant loading down the long axis of the implant.
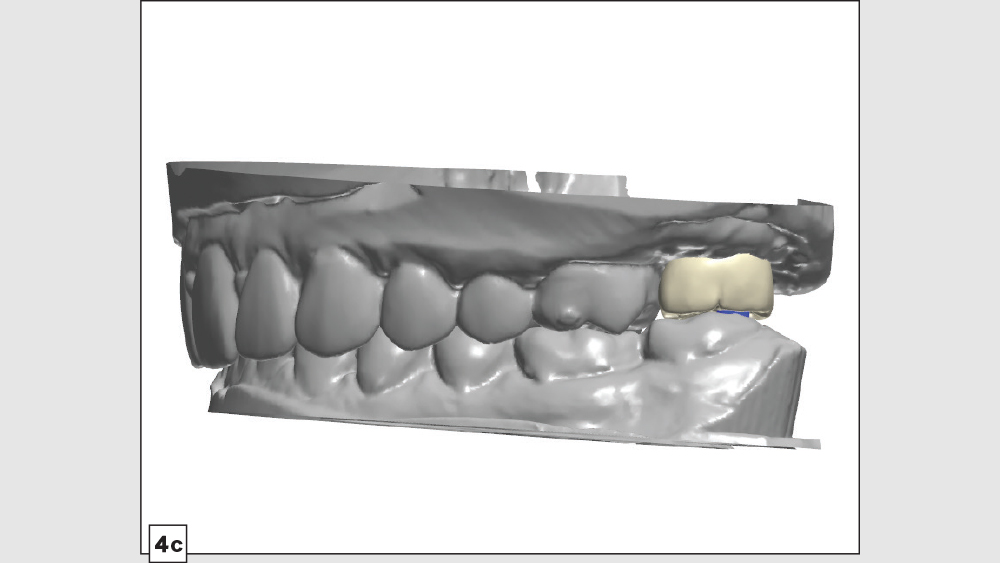
Figures 4a–4c: The custom abutment was digitally designed with an ideal emergence profile, correcting for the nonideal position of the implant while replacing the restorative material cantilever of the prior restoration with titanium contoured to minimize shear forces. The crown was designed with a narrow occlusal table and minimal cuspal heights to direct implant loading down the long axis of the implant.

Figure 5: An Inclusive® Titanium Custom Abutment and BruxZir Full-Strength crown were milled from the CAD design. The crown for a screwmentable restoration is designed the same way as a traditional crown over custom abutment, with the exception of the screw access hole.

Figure 6: At the final delivery appointment, the custom abutment and crown were tried in to verify accurate fit, contacts and occlusion. The restoration was then removed so the crown could be cemented to the abutment outside of the patient’s mouth. To begin, Teflon™ tape was used to cover the screw access channel and keep any cement from entering the implant-abutment connection. Note that VPS or any other suitable material can be used for this purpose.
Figure 7: After cleaning the abutment surface and the intaglio surface of the crown, RelyX™ Unicem 2 (3M™ ESPE™; St. Paul, Minn.) was used to cement the crown to the custom abutment.
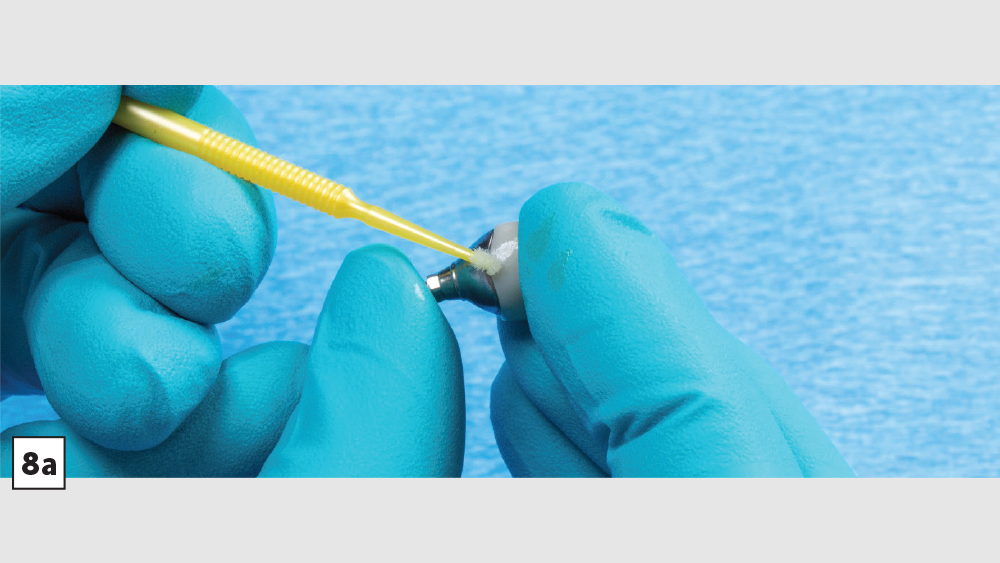
Figures 8a, 8b: A microbrush was used to clean away cement from around the margins of the custom abutment and implant crown. The newly one-piece restoration was carefully inspected to ensure that all excess cement was removed. After light-curing the cement, the Teflon tape was removed from the screw access channel.

Figures 8a, 8b: A microbrush was used to clean away cement from around the margins of the custom abutment and implant crown. The newly one-piece restoration was carefully inspected to ensure that all excess cement was removed. After light-curing the cement, the Teflon tape was removed from the screw access channel.

Figure 9: The custom abutment and crown were now ready to deliver as a one-piece, effectively screw-retained restoration. The screwmentable crown resulted in an improvement in emergence profile and reduced the restorative material cantilever of the patient’s prior restoration.

Figures 10a, 10b: The final one-piece restoration was seated and delivered as a screw-retained crown. With the improved distribution of functional forces, cleansability and support provided by the custom abutment, the screwmentable restoration has established the foundation needed for favorable long-term health of the implant site.
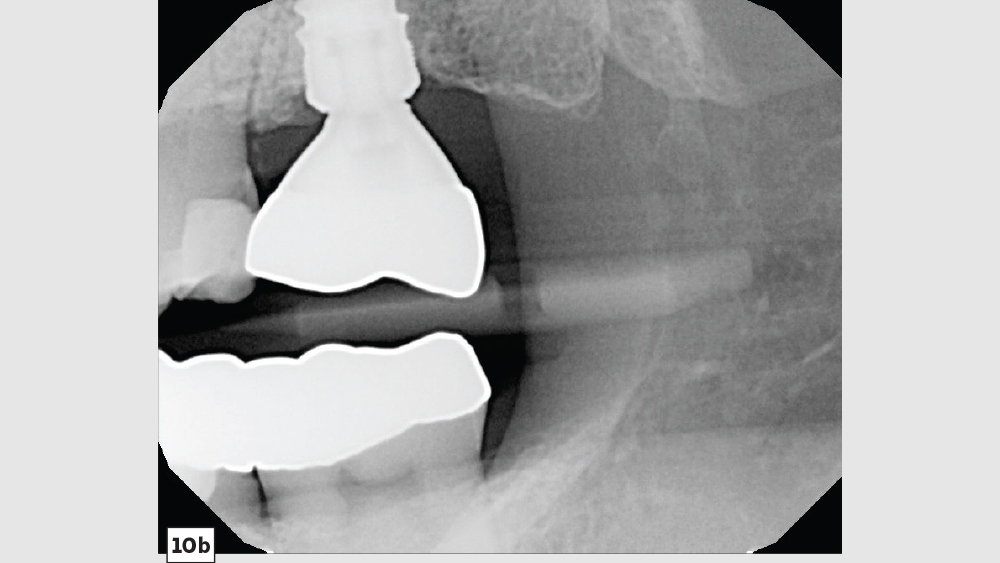
Figures 10a, 10b: The final one-piece restoration was seated and delivered as a screw-retained crown. With the improved distribution of functional forces, cleansability and support provided by the custom abutment, the screwmentable restoration has established the foundation needed for favorable long-term health of the implant site.
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
CONCLUSION
When determining the optimal type of restoration for an implant case, it is important to consider functional forces, emergence profile, ease of delivery and the potential for prosthetic complications. While screw-retained crowns and cementable restorations over custom abutments both offer certain advantages depending on the circumstances of each case, there are unique situations and restorative challenges that call for a screwmentable solution, affording clinicians one more option as we look to meet the wide-ranging needs of our patients.
NOTE: To prescribe a screwmentable restoration through Glidewell Laboratories, select a custom abutment with crown when you fill out your prescription, and request an access hole in the crown in the case notes. The Implant Fixed Rx can be downloaded here or requested by calling 800-757-4428.
References
- ^Wadhwani C, Piñeyro A. Technique for controlling the cement for an implant crown. J Prosthet Dent. 2009 Jul;102(1):57-8.
- ^Wadhwani C, Rapoport D, La Rosa S, Hess T, Kretschmar S. Radiographic detection and characteristic patterns of residual excess cement associated with cement-retained implant restorations: a clinical report. J Prosthet Dent. 2012 Mar;107(3):151-7.
- ^Wadhwani C, Hess T, Piñeyro A, Opler R, Chung KH. Cement application techniques in luting implant-supported crowns: a quantitative and qualitative survey. Int J Oral Maxillofac Implants. 2012 Jul-Aug;27(4):859-64.