
In this issue:
One-on-One Interview with Neil Park, DMD
Interview by

Interview with


Dr. Neil Park is the new director of clinical affairs at Glidewell Laboratories, where he oversees the clinical aspects of product research and development, and helps guide the company’s practitioner training and education efforts. Dr. Park also serves as a managing editor for Chairside® magazine. Here, he discusses what motivated him to leave his private dental practice for a career in the manufacturing side of the industry, his role in developing implant curriculums in dental schools across the country, the learning curve today’s graduates face in the field of implantology, and more.
DAVID CASPER: I want to dive into your background, but I want to start with what made you decide to go to dental school. How did you become a dentist?
DR. NEIL PARK: Dave, I hope you’re not expecting some kind of enlightening, inspiring or even interesting story because it doesn’t go like that. The true story is that when I was a senior in high school in Miami, we had four guys that had a car pool together. Three of us drove these broken-down, beat-up, old cars, and one of the guys pulled up in a really nice Pontiac Bonneville convertible with leather upholstery. That guy’s father was a dentist, which got the rest of us very interested in the field of dentistry. In fact, three of those four guys are now dentists.
But on a more serious note, I didn’t have anybody in my family that had previously been involved in dentistry. So all I knew about dentistry was what you know as a patient, which isn’t very much. When I was an undergrad at Bucknell University, I went for my recall visit during one of my trips home to Florida and had a nice heart-to-heart with my dentist, who was very supportive of me getting involved in dentistry. He gave me a lot of advice about the education requirements and the great lifestyle that you can potentially have as a dentist, as well as the other things that go with it: bringing smiles to people and really improving their quality of life.
DC: Fantastic. So you went to Temple University for dental school, correct? How did you choose that school?
NP: That’s right, and it was kind of a cost-based decision. I had just finished college in Pennsylvania, and I was accepted to Temple and to the University of Pennsylvania. Penn has an incredibly wonderful dental school, but it was a private school and had very high tuition. Temple is a state school, so the tuition was much lower. I got a good education and came out a little bit less encumbered than I might have otherwise.
DC: Was there any dental implant curriculum or courses in dental school for you?
NP: There was very little. I remember in one lecture the basic information that I received was: Dental implants are really bad, and, if you’re an ethical practitioner, you’ll stay far away from them.
DC: So did you go into private practice after you graduated?
NP: I was in private practice for 12 years.
DC: And then you began a great career working for some of the largest market-leading companies in the dental implant and dental technology space. What made you decide to get out of private practice and come to this side of things?
NP: When you first go into practice you have all this debt from your education and then you layer on top of that the debt to start a new practice. So for those first 12 years of private practice, I really didn’t have a lot of options. You go to work and you make your practice successful and there really isn’t a lot of taking stock of what you’d like to do.
After those 12 years, when the financial burdens were lifted and the practice was successful, I took a hard look and said, “What kinds of things do I really enjoy doing, and how do I want to map out the rest of my life?” And I really felt like I enjoyed getting out with people. I enjoyed speaking in public. I enjoyed negotiating with people about different things. So I made the somewhat questionable decision to go to law school. I sold my practice and, normally, when a practice is for sale, it’s sort of on the downswing, right? It’s an older doctor whose practice hasn’t been growing. But since my practice was still on the upswing it sold very, very quickly.
I had a few months before law school would be starting, and at that point the leading company in this very new field of dental implantology recruited me. So I thought, “OK, I’ll go to work for them for a few months until law school starts.” But from the moment I got involved in the industry I just loved every minute of it. It was exactly what I was looking for. It was the opportunity to work with people who had talents very different from mine, people who I could learn from. The biggest thing to me was this new technology, these osseointegrated dental implants. This had the capacity to change the practice of dentistry and, more importantly, to change people’s lives more than anything else that I’d seen come along in dentistry.
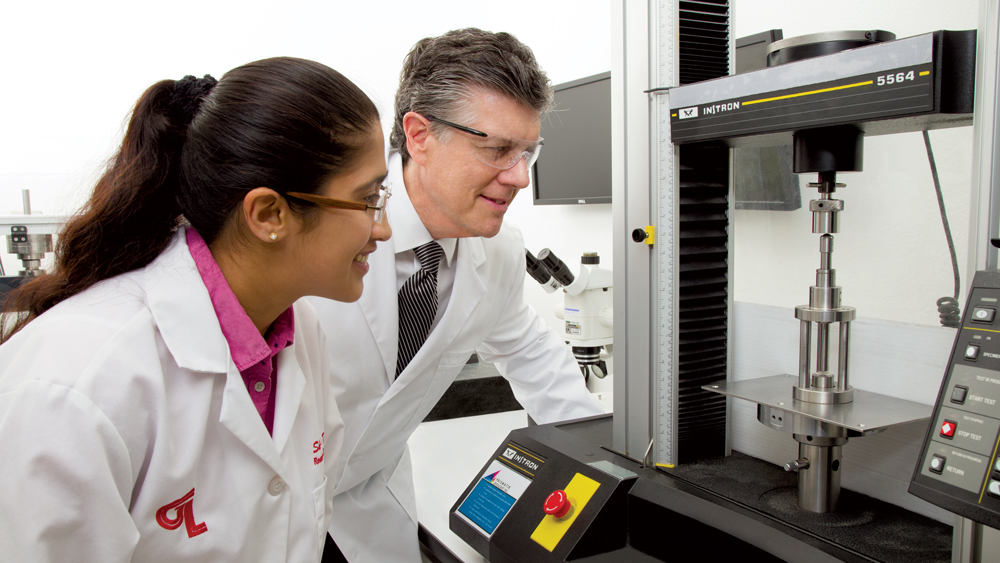
Dr. Park and Research Associate Shreya Shah observe a fracture toughness test at the Glidewell Laboratories R&D facilities.
DC: Before diving into dental implants, I want to go back to something you just said related to dental students graduating with a lot of debt and a big financial burden. We hear that a lot today. Do you think that, in any way, contributes to the rise in the DSO (dental service organization) space, these group practices, corporate dentistry? There seems to be so many graduates that start there.
NP: That’s right, and I think it’s good that there is a place to go for the young graduate who needs to start earning money right away. Typically, if you open a private practice or become an associate in a small private practice, it takes a while to get your income to a reasonable level. DSOs offer a great opportunity for people to get out there and start seeing patients right away. They often have a salary so that they can sort of get their act together and decide how they want their career to look for the rest of their lives. And some of the large DSOs have training programs; they have a career path for these young doctors to gain more clinical skills while they better their financial situation.
DC: Let’s tie that into your comment about dental implants and dental implant technology. What’s your take on the general dentist’s access to implant training today? Has it improved since your days at Temple? Are there formalized curriculums now?
NP: I was very fortunate to be involved in the support the industry provided in changing the core curriculum in dental schools so that, in most cases, predoctoral students now have a really nice introduction to dental implants.
It really started around 2005. The deans of the U.S. dental schools got together, had a meeting, and decided that they would commit to making dental implant treatment part of the core curriculum for predoctoral students. So I was part of a group of companies that assisted with this. We assisted with curriculum development, parts and pieces, and the things that needed to be done to get the program up and running.
So, as opposed to when I came out of school, when there was either no information at all or very poor information, at this point it’s very different. The young dentist coming out of school today will have had a lot of lectures and the opportunity to do some simulation exercises in a laboratory. They’ve also most likely treatment planned and restored some cases, though most have not had the opportunity to place implants.
DC: What do you think is needed for the dentists that are graduating today? They’ve at least had some exposure at the undergraduate level, but if they go into private practice, a recent statistic said that up to 40 percent of these dentists end up in a DSO for at least 24 months. While that’s great from a patient care perspective, how do they then make the transition into learning more about implants and truly incorporate that indication or that method into a private general dental practice?
NP: One of the big differences with today’s graduate is that in most cases they have the expectation that they will be involved in the surgical placement of dental implants at some point in their career.
DC: It’s inevitable.
NP: It’s inevitable; that’s where they’re going to go. In the predoctoral curriculum there just really isn’t time to go into the surgical aspects of it, but they’ve had some good grounding in treatment planning and the restoration. So then it’s really left up to that graduate to find a pathway to learn the skills, to learn the information, and to get the practical experience needed to provide this treatment.
DC: Is there typically something in your experience that makes the dentist decide, “Hey, now I’m ready for this”? Is it experience-based? Is there an educational component to that? What makes one decide now is the time to dive in?
NP: A lot of times it’s just simply that a good educational opportunity presents itself. There are also situations where people have had practice analyses done that look at the procedures that they do and say, “You know, you’re extracting a lot of teeth, you’re doing a lot of partial dentures, you’re doing a lot of removable dentures, and there’s some additional care that your patients would benefit from that you’re really not recommending.”

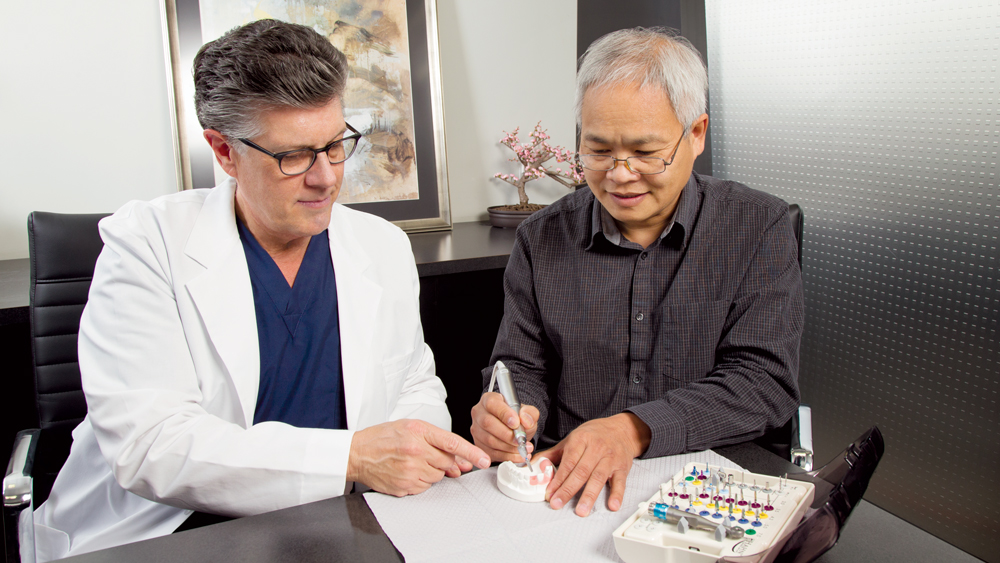
Dr. Park discusses implant prosthetics with Glidewell Laboratories Vice President of R&D Akash (left) and R&D Manager Tom Valenti (right).
DC: We’ve had a number of clinicians sit in that very chair and I always ask the same question: “What made you decide to place that first implant?” More often than not it’s that a given patient came in and said, “I want you to do it.”
NP: Exactly.
DC: And that’s when they made the decision to learn.
NP: Many dentists have been dragged kicking and screaming into dental implantology, and that’s a good thing as long as they can get the right training. And right now there are a lot of choices in getting this kind of training. There are industry-sponsored programs, and there are several very strong freestanding educational institutes that provide this training. They also have choices on the format. There’s the shorter, say, two-day type of format, and then there’s the longer format that goes a full year.
DC: A much deeper dive.
NP: Yeah, and there are a lot of good opportunities for the doctor who’s willing to invest the time and the money to get this training.
DC: Which is a good thing, right?
NP: It is.
DC: Let’s switch back to the dental implant industry. You mentioned earlier that instead of law school you decided to go work for one of the leading dental implant companies. Back then there were something like five dental implant companies selling implants in the U.S., and now there are 100 or whatever the number is. Why is that? Does the world need that many dental implant systems? Are these companies so significantly different from each other? What’s driving this expansion at the product level?
NP: I think part of it is a price umbrella that’s been created by the premium companies. They’ve set a retail price that’s pretty high, and other companies think, “Gee, we can make a product that is similar.” In many cases you see these sort of knockoff products that are priced less. They don’t have the R&D involved, and they don’t provide some of the other services that are of value to some doctors, but may not be of value to other doctors. So there’s this fragmentation in the industry. There’s the premium tier, there’s the mid-level tier and then the value tier. Most of it’s based on what kinds of ancillary services the doctors would like to have or require in order to make their practices grow in the direction they want.
DC: Right. You mentioned R&D earlier. It’s interesting, I think back to when you and I were selling implants a long time ago and there were really only half a dozen companies or so. It was all implant surface wars and documentation and research and development to really justify that one product works better than the next guy’s. But today, there’s just an assumed position that they all basically work. Do you think this is good or bad?
NP: That’s right. There’s an assumption that the product is safe and effective, and then it’s a question of which particular features the doctor prefers. Of course, there are very strong opinions based on preservation of crestal bone, the preservation of hard and soft tissue; that’s what it’s all about. And some of that relies on technique, and some of it relies on implant design. Doctors have a wide range of choices in getting what they think will work best.
DC: Yeah, I agree with that very much. You mention tier-one and tier-two companies. If you look at the market leaders that have historically held the bulk of the market share, it seems to me there’s an increasing trend that I would call “different sameness” related to these companies. You have traditional market-leading companies that were big in, let’s say, tissue-level implants introducing a bone-level or a two-stage implant.
NP: Exactly.
DC: And vice versa, the No. 1 or the No. 2 is now: “Well, I didn’t have that. I’m going to add this.” Is this just noise, or is it expanding the existing customer base? What impact is that having?

Dr. Park and Shreya Shah evaluate test results to determine the strength of a prosthetic material under development at Glidewell.
NP: I think at this stage of the market, at this level of development, it’s rarely about the product. What defines market leadership is defining a specific technological advancement and then bringing that forward. I think an example would be All-on-4.
When All-on-4 was first promoted it was put together as a really good, effective way for a dentist to provide immediate load, full-arch cases for people that badly needed it. The company that promoted All-on-4 and brought it out in an educational method did a lot of good for the market, and I think you know that’s where we are right now in the industry. It’s about finding a solution and the solution definitely uses certain products, but it’s not 100 percent product-dependent.
DC: I think the company you’re referring to is ClearChoice. I had an interesting conversation with Dr. Mark Adams, the Vice President of Clinical Affairs at ClearChoice, not so long ago and he talked about how, in the beginning, or early on in implantology, everyone was doing full-arch cases and then there seemed to be this lull where you would talk to dentists and even specialists who would say, “Well, I don’t see many of those patients anymore.”
NP: Yeah.
DC: And since ClearChoice made its entrance into the marketplace with its direct-to-consumer advertising, now everybody is doing full-arch cases. Were those patients just missing for a while? Or they disappeared and came back? Is it really the outreach to the patient directly, or is it something else?
NP: Dave, as you know I had the good fortune to spend a couple of years with the ClearChoice team, and what’s really interesting is that the patients who are having this full-arch edentulous treatment don’t come in as edentulous. Those patients come in with terminal dentition — the guy that’s been walking around suffering from advanced periodontal disease, advanced dental decay, lots of missing teeth, unattractive smile, lack of confidence, and all those lifestyle issues that come with it. These patients didn’t know what to do, and what ClearChoice did was this direct-to-consumer advertising that showed them that there is a solution to this problem and where to get it. They also gave a very convenient treatment and buying experience to the patient.
DC: Right. Is that patient you mentioned, though, not going to a general dentist regularly? Is that why he hadn’t been exposed to this information?
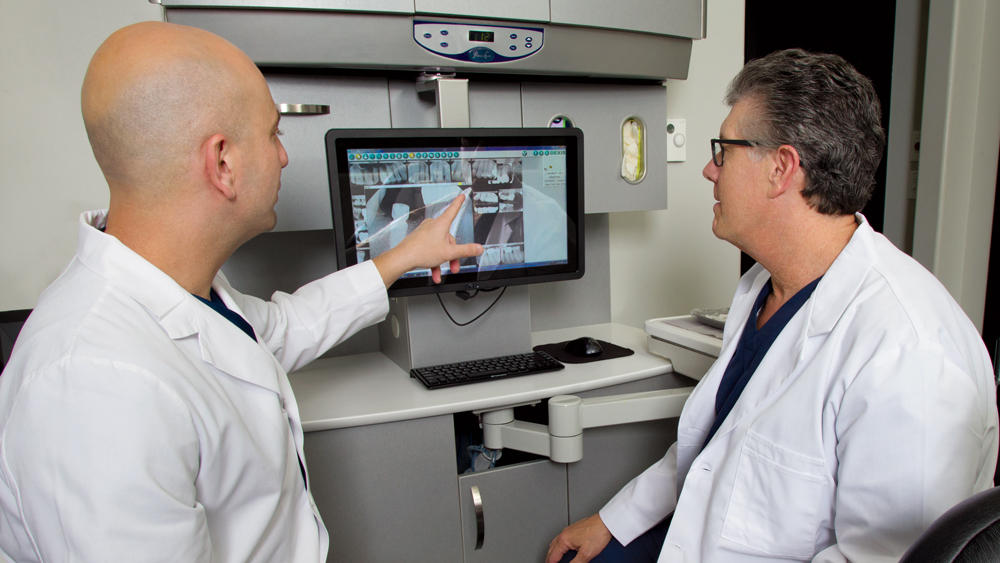
Director of Clinical Research and Development Dr. Siamak Abai discuss an implant case with Dr. Park at the Glidewell International Technology Center operatory.
NP: That’s right. I think you said that the doctors weren’t seeing those patients. Well, you could also say those patients weren’t seeing the doctor. And in many cases these are people that haven’t been to a dentist for 10 years or more, or maybe they’ve just had some extractions on occasion as needed.
DC: That’s interesting. We’ve talked about All-on-4 being a solution that’s presented and ultimately resulted in the ClearChoice business model, if you will. What’s next in that space? I think that we, collectively as an industry, need the market leaders to in fact drive the market, to expand options and to get more dentists in the pool. It’s such a deep pool, even today. There’s so much opportunity in front of us.
NP: Absolutely.
DC: In your view, what’s next on the horizon?
NP: It’s the improvement of the workflow. Right now there are so many different entry points for a doctor wishing to do cases like this. There are different entry points for the patient, and there are different entry points for the doctor. All the pieces are there now. We have the availability of 3D imaging that gives doctors such a rich visual of what’s going on in the patient. This allows them to go into the operating room with so much more knowledge about what they’re going to face and how to deliver better care to the patient. So the parts and the pieces are there: intraoral scanning, CAD/CAM and all the great things we can do with design. All those parts are there, but the workflow isn’t there yet, and I think that’s the big advancement that’s coming.
DC: Right. And so many people we talk to mention guided surgery as an example of a tool — and maybe the most significant tool — to get the general dentist comfortable with the surgical placement of a dental implant. Why isn’t everybody doing that? Is it the cost associated with guided surgery? Is it the workflow that you mentioned? What’s preventing this from just becoming the standard, if in fact it would have that much impact on the business?
NP: Guided surgery is a tremendous technical advancement and it certainly has its place, but what I’ve found is that guided surgery depends 100 percent on the availability of 3D imaging.
DC: Right. Cone beam.
NP: What I’ve found is that when doctors have those 3D images available to them, they say, “OK, I’ve got this rich data set now, I know what’s coming, and I don’t need to have guided surgery quite as often as I thought I was going to need it.” So it still has its place, but it’s not a substitute for training, experience and planning.
DC: So you’re saying guided surgery trains the dentist to not need guided surgery.
NP: Let’s say a doctor purchases a CBCT scanner so he could do guided surgery. He may find that he doesn’t need to do guided surgery now that he has the CBCT.
DC: Interesting. So it’s an expensive investment that will at least get the dentist involved maybe sooner in their career; so that’s not necessarily a bad thing.
Dr. Park assists a doctor with the Hahn™ Tapered Implant System during a course at the Glidewell International Technology Center.
NP: And it’s a great way to practice. It does give tremendous information, but it’s not a required prerequisite for delivering good care.
DC: Let’s go back to education for a second, as we recently announced a strategic partnership with Dr. Carl Misch and Misch International Implant Institute. Have you had any experience with Dr. Misch? What’s your opinion there?
NP: Everyone in our industry knows Dr. Carl Misch. He’s truly one of the giants, and he has contributed as much as anybody to the advancement of dental implantology. I mean, my goodness, he’s written the two most popular textbooks — the two standard textbooks in dental implantology. But I think he might agree that his greatest legacy is probably the Misch Institute. In the years that you and I have been in this field, I have to say that whenever I meet a general dentist who has a growing, really successful private practice and does a lot of implants, that doctor was invariably trained at the Misch Institute. They’ve put together a program that does everything from a biological perspective. Carl always talks about how implantology is not carpentry, how you have to have an understanding of treatment planning that’s based on biology and biomechanics. Then, of course, there’s all the skills required to place implants and restore them successfully. So it’s a yearlong continuum; it’s a tremendous program. It’s absolutely the top in the industry.
DC: Definitely. We’re really proud and looking forward to being a part of it. Let’s talk about your new job as director of clinical affairs here at Glidewell Laboratories. For readers who haven’t had the chance to visit us, we have a number of clinicians and a number of operatories all working in a research and development capacity here at the company. And we’ve charged Dr. Park with leading that group and coordinating our efforts. What’s on your agenda here early on?
NP: The secret to success in putting together any program in our industry is to focus on the needs of the doctor. I’ve had what is perhaps a unique background including some years of private practice and then some years in the industry. My goal is to take that experience and bring it to our dentist customers so they can incorporate new technologies into their practice, be more successful, and offer more services and more successful treatment to their patients. That’s really what I want to do here.
As you mentioned, we have such a unique situation here at Glidewell Laboratories. We have 77 scientists in our R&D department and we have a team of four dentists, so we have a sort of closed feedback loop. We can come up with a product idea, we can test it, we can do a clinical study, and only then, when we know that it works, we can launch it to our dentist customers. I think it’s a rare opportunity, and it’s very exciting to see what we can do to advance dentistry.
DC: Yeah, we agree. Glad you’re here, sir. Welcome to the team.
NP: Thanks, Dave.