In this issue:
Tapered vs. Parallel-Walled Implants: Which Is the Better Design and Why?

Note: The Hahn Tapered Implant System is now known as the Glidewell HT Implant System
The design of the dental implant body — or macrostructure — is the key design feature in achieving primary stability, which is the main prerequisite for achieving successful osseointegration of dental implants. This is particularly critical in areas of poor bone quality (D4 bone), which are associated with increased morbidity and lower success rates. Despite the importance of this design feature, there have been few studies comparing the performance of tapered implants vs. parallel-walled implants in poor-quality bone.
To address this knowledge gap, Dr. Christopher Resnik recently conducted a study to examine whether tapered or parallel-walled dental implants provide greater primary stability. Due to the increasing popularity of immediate loading of dental implants, which relies on initial stability, he set out to determine if there is a specific implant design that can be used to increase clinical success.
Dr. Resnik is a prosthodontist in private practice in Winter Park, Florida, and recently graduated from the specialty training program in prosthodontics at the University of Pittsburgh, where he conducted this study. His father, Dr. Randolph Resnik, is the director of the Misch International Implant Institute, which has set the standards for dental implant education for over 30 years. Dr. Christopher Resnik’s new study, which has been accepted for publication, is the first of its kind, and its findings have important implications for clinicians. Here, we’ll discuss implant body design and present a summary of this exciting new research.
Figure 1: Dr. Christopher Resnik (second from right) joined by his sister, Allison, and parents, Randolph and Diane Resnik, while receiving his Diplomate status from the International Congress of Oral Implantologists.
DISCUSSION
Implant Body Design
Implant designs include cylindrical and threaded types. However, implants with a threaded design predominate due to their increased surface area, which allows for increased bone-implant contact (BIC) and more predictable integration. Increased BIC is associated with superior primary stability and minimal micromotion, which is paramount to success.1
Threaded implants may be either parallel-walled (equal diameter along the entire implant body) or tapered (decreasing diameter toward the apex, similar to a tooth root). Tapered implants divert forces toward the apex, making this type of implant more desirable for immediate placement and immediate loading.2 Tapered implants have also been shown to distribute occlusal forces to adjacent bone more favorably than parallel-walled implants.3
Dr. Jack Hahn is recognized for pioneering the first tapered implant in the 1990s and for developing the Hahn™ Tapered Implant in 2015. Tapered implants require less bone volume at the apex due to the decreased apical diameter. Therefore, they are less likely to perforate the cortical plates when osseous undercuts are present in the regional anatomy. In addition, they are ideal for implant sites with compromised space between tooth roots.

Figure 2: Cylindrical dental implant.


Figures 3a, 3b: Threaded implant: Parallel-walled design (3a) vs. tapered implant (3b).
Figure 4: The design of the Hahn Tapered Implant, shown above, is advantageous in anatomically constricted sites, as well as in sites planned for immediate loading. Clinical photo courtesy of Dr. Jack Hahn.
Primary Stability and Osseointegration
Primary stability is the initial mechanical fixation of a dental implant immediately after placement within the bone. Primary stability of the dental implant is crucial in obtaining osseointegration.4 This stability directly affects the rigidity and resistance to movement of the dental implant before the initiation of the bone remodeling and healing process. Studies have shown that micromovement greater than 150 µm is detrimental to osseointegration5 Therefore, prevention of micromovement is essential in averting early implant failures.
The tapered design has been shown to provide greater lateral compression of the bone during insertion.6 This could lead to an increase in primary stability, favoring tapered implants to be used in sites with poorer bone quality or inadequate bone volume, and in sites planned for immediate loading.
STUDY SUMMARY
It was hypothesized that placement of tapered implants in poor-quality bone would demonstrate a higher degree of initial stability than parallel-walled implants placed in the same medium. This, in turn, could lead to greater osseointegration and implant success.
To determine which type of implant provides greater primary stability, Dr. Resnik collaborated with Grant Bullis, vice president and general manager of the Manufacturing division at Glidewell, to fabricate a parallel-walled prototype implant to compare with the Hahn Tapered Implant. In all other characteristics, the implants were identical, including the same titanium alloy, implant length and diameter (4.3 x 13.0 mm), implant collar, and thread design. The only difference between the tested implants was the macrostructure: tapered vs. parallel.

Figure 5: For the study, the lab fabricated test implants with identical design characteristics. The only difference was the wall design, with the tapered-body Hahn Tapered Implant (left) and parallel-body prototype (right).
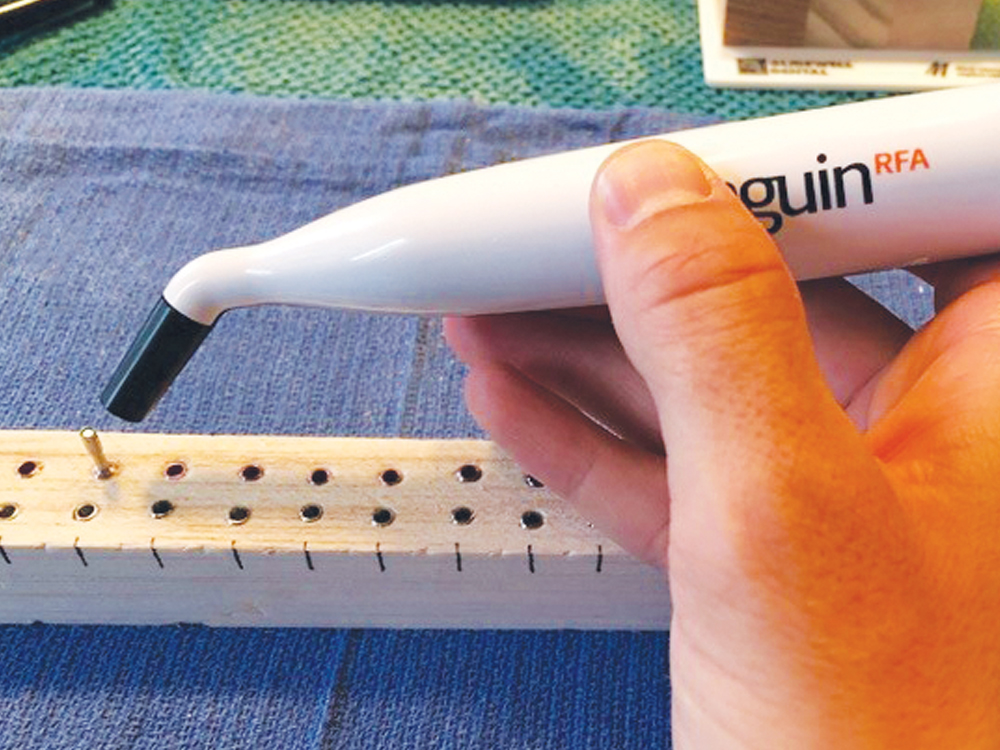
Figure 6: Resonance frequency analysis recording using Penguin RFA.
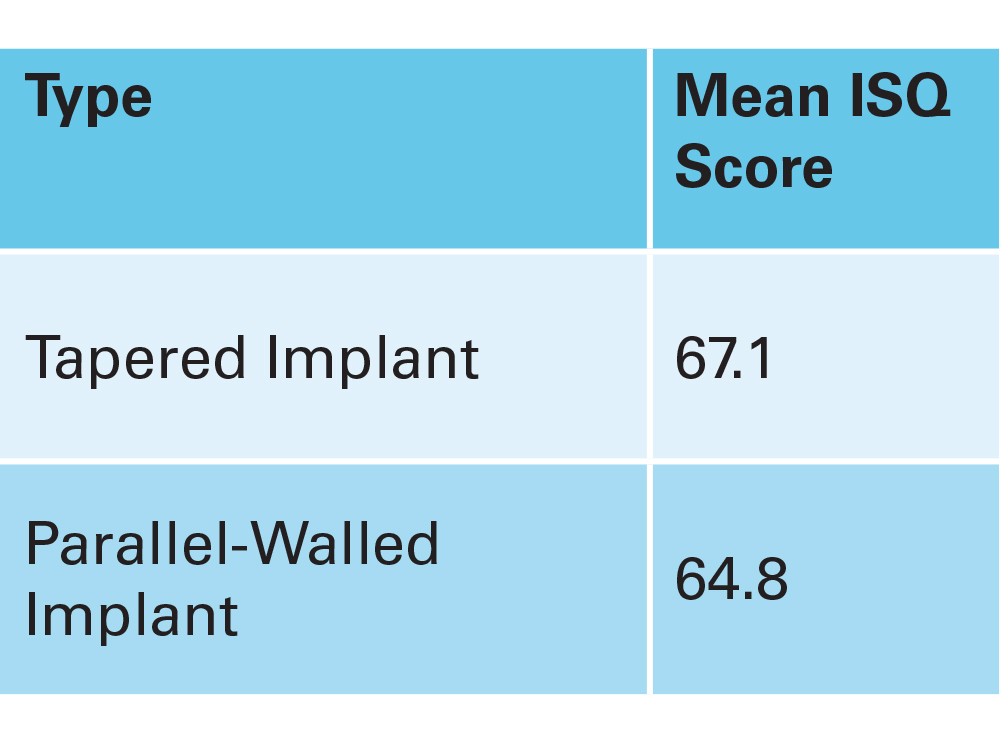
Figure 7: ISQ results for tapered vs. parallel-walled implants. The study concluded that tapered implants achieve significantly greater primary stability.
Twenty-four tapered and parallel-body dental implants were placed fully guided with a drill press into a poor-quality bone medium (balsa wood). The primary stability of each implant was evaluated using resonance frequency analysis with the Penguin RFA® (Glidewell; Irvine, Calif.). Implant stability quotient (ISQ) scores, which correlate to primary stability, were calculated and compared for each implant.
The mean ISQ value for tapered implants was 67.125 +/- 1.974, and the ISQ value for parallel-walled implants was 64.813 +/- 0.93. The study concluded that tapered dental implants reach a statistically significant greater primary stability in poor-quality bone than parallel-walled implants.
CONCLUSION
Implant body design is of critical importance to the success of implant treatment, particularly in sites with poor bone density. Although past studies have been conducted to evaluate different implant designs, this study is believed to be the first to compare a parallel-body implant vs. a tapered implant with all other variables of implant design kept identical.
The study found that tapered implants provide greater primary stability than parallel-walled implants. This is important because primary stability is a key prerequisite for successful osseointegration. With the popularity of immediate loading protocols in implant dentistry, the implant surgeon can increase predictability and success by selecting a tapered implant.
References
- ^ Watzak G, Zechner W, Ulm C, Tangl S, Tepper G, Watzek G. Histologic and histomorphometric analysis of three types of dental implants following 18 months of occlusal loading: a preliminary study in baboons. Clin Oral Implants Res. 2005 Aug;16(4):408-16.
- ^ Morris HF, Ochi S, Crum P, Orenstein IH, Winkler S. AICRG, part 1: a 6-year multicentered, multidisciplinary clinical study of a new and innovative implant design. Oral Implantol. 2004;30(3):125-33.
- ^ Glauser R, Sennerby L, Meredith N, Rée A, Lundgren A, Gottlow J, Hämmerle CH. Resonance frequency analysis of implants subjected to immediate or early functional occlusal loading: successful vs. failing implants. Clin Oral Implants Res. 2004 Aug;15(4):428-34.
- ^ Albrektsson T. Direct bone anchorage of dental implants. J Prost Dent. 1983 Aug;50(2):255-61.
- ^ Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. J Biomed Mater Res. Summer 1998;43(2):192-203.
- ^ Atieh MA, Alsabeeha N, Duncan WJ. Stability of tapered and parallel-walled dental implants: a systematic review and meta-analysis. Clin Implant Dent Relat Res. 2018 Aug;20(4):634-45.
Penguin RFA is a registered trademark of Integration Diagnostics Sweden AB.