In this issue:
My First Glidewell HT™ Implant with John Geasland, DDS
Interview with


Note: The Hahn Tapered Implant System is now known as the Glidewell HT Implant System
Dr. John Geasland is an experienced dentist practicing in Tahlequah, Oklahoma, who made the leap to implant surgery after 20 years of general practice. In this interview, he explains why he decided to begin placing implants, why annual CE requirements present an excellent opportunity to learn about implants, and what led him to recently adopt the Hahn™ Tapered Implant System in his practice.
CHAIRSIDE® MAGAZINE: As a general dentist, what initially sparked your interest in placing implants?
DR. JOHN GEASLAND: When I was in dental school, implants were not part of the general dentistry curriculum, but I was allowed to watch procedures being performed by residents in the oral surgery department, and I thought it was really interesting. That was back in 1986, a few years before implants entered into the mainstream. I’d see the cases and ask a lot of questions, and it was clear that implants were the best solution for solving the problems of missing teeth. I thought it was really great how, instead of cutting teeth down for a 3-unit bridge, you have the option of replacing a tooth without damaging the adjacent dentition or using a removable appliance.
CM: How long ago did you place your first implant?
JG: The first implant I placed in a patient was about 10 years ago. By then I had learned that implant dentistry is a prosthetically driven discipline with a surgical component, and that many restorative issues are prevented if the surgeon is thinking about the prosthetic outcome. So when I started placing implants, I learned early on that I shouldn’t simply place the implant where bone is thickest, but rather in an ideal position for the restoration.

Dr. John Geasland began placing implants 10 years ago after discovering that many patients were hesitant to follow through on referrals and would strongly prefer to receive the full circle of treatment within his practice.
CM: What made you finally decide to start placing implants?
JG: One of the main reasons I started was because I had patients who wanted implants but were looking for a one-stop shop. They were not following through with my referrals to the specialists, and they’d tell me, “I wish that you could do it.” Their trust was with me, not the doctor I referred them to, so I figured I should learn this for the sake of my patients. A question I would often get was, “You mean I have to drive 30 minutes away?” These patients did not want to travel to receive treatment. So I started placing a few here and there, and it quickly became an important part of my practice.
CM: How did incorporating implant surgery affect your practice and the treatment you provide your patients?
JG: We were able to keep the continuity of care a lot smoother, and maintaining a restorative-driven approach was a lot easier because I was responsible for my own treatment planning and implant positioning. Patients would follow through with treatment more often and with less hesitation. This helped my entire practice and increased the case acceptance rate for implant treatment, which of course comes with some additional revenue. It has certainly helped my private practice in competing against large corporate dentistry.
CM: What led you to giving the Hahn™ Tapered Implant System (Glidewell Direct; Irvine, Calif.) a try?
JG: I was using BioHorizons® implants a few years ago when I saw an interview with the late Dr. Carl Misch where he endorsed the Hahn implant, and I thought it sounded like an interesting implant system. Dr. Misch invented one of BioHorizons’ most popular implants, so if he was moving over to the Hahn Tapered Implant, there must have been something to it.
I’ve watched a lot of Glidewell Dental training videos like “Chairside Live” over the years, so I decided to attend a training taught by Dr. Charles Schlessinger in Oklahoma City so I could try out the Hahn implant. Attending that course made switching to the Hahn implant system accessible and affordable. There were hands-on exercises and I really liked how the system works.
The cost of the implants was much lower than BioHorizons, and I really liked the one-stop shopping with Glidewell Direct. The package deal that Glidewell offers, where you get the surgical and prosthetic kits for free, really worked for me. And the affordable cost and technical support I receive have been very helpful for my practice. There’s always someone available to answer any questions I have, and I’ve even received helpful responses after sending emails to Drs. Tim Kosinski and Paresh Patel, who teach courses for the Glidewell International Technology Center. I’ve never experienced that level of support with the other implant systems I’ve used.
CM: Can you discuss your first experience placing a Hahn Tapered Implant? What kind of case was it?
JG: My first was an upper central incisor. With my previous surgical kit, I would have had to reverse the implant out of the bone and put it back in. But with the Hahn implant, because it’s self-tapping and has those deep, sharp threads, I was able to go ahead and position the implant 1 mm deeper after realizing this was needed to avoid showing metal. I just gave it a little more torque, and it went right into position. The implant design solved a moderate problem with a simple, easy adjustment.
So that first experience was great, but the case I want to share is an interesting two-implant case I recently did to replace a single molar. The tooth could have been restored with a root canal, post and core, and crown, but implant treatment offered a better long-term prognosis and was the patient’s preference after learning of her options. We went with two 3.5 mm x 11.5 mm Hahn implants because the buccal-lingual bone width was too narrow to accommodate a larger implant and placing one implant of that size would have made the crown look like a lollipop. The biomechanics wouldn’t have been great either, so we went with two medium-sized premolars, which also resulted in better hygiene. I extracted the tooth, grafted the socket with Newport Biologics™ Mineralized Cortico/Cancellous Allograft Blend (Glidewell Direct), and placed the implants four months later.
CM: Did the surgical procedure go as you expected?
JG: The surgical procedure went very smoothly, like clockwork. There were no surprises, and the implants threaded into place very nicely. One of the things I like about the Hahn system is that the osteotomy drills account for the full body of the implant and create the precise amount of space you need. Other implant systems force you to jam the implant into virgin bone because the rounded corners of the implant are not accounted for in the shaping drill. And because they’re not self-tapping like the Hahn implant, this complicates things a bit. The Hahn implant system is very streamlined and makes for a more accurate fit between the osteotomy drills and the implant, using a very straightforward drilling sequence. You pick up on that within the first 10 minutes of looking at the surgical kit, which is very well thought out.
CM: Was the patient happy with the outcome?
JG: She was very happy with how the restorations looked and, like most of my patients, she appreciated being able to receive the full circle of care in my practice.
CM: So you’ve decided to make the Hahn implant your system of choice?
JG: I’m now using it full time and have not seen the need to use anything else, whether I’m doing a single unit, an extraction with immediate implant placement, or a full-arch case. The 3.0 mm implant has certainly been helpful in overdenture cases where I don’t have an ideal amount of bone.
CM: As a general dentist, how do you decide which cases to refer out for implant surgery?
JG: If the patient is high-risk or has a history of healing problems, I tend to refer the case to a specialist. Also, if there is not ideal bone volume or density, I’ll refer it to a specialist. If the patient follows through, the surgeon will place the implant, and we work together to make sure we get the best possible prosthetic outcome.
CM: Would you recommend that other practitioners give the Hahn Tapered Implant System a try?
JG: I would recommend it because the whole system is so accessible and easy to use. And then you have the people at Glidewell to help you with any restorative questions you have during the planning stage. Having that technical support for both the surgical and prosthetic components of implant dentistry is really wonderful.
The whole system is so accessible and easy to use. And then you have the people at Glidewell to help you with any restorative questions you have during the planning stage. Having that technical support for both the surgical and prosthetic components of implant dentistry is really wonderful.
CM: What kind of training do you recommend for the GP who is looking to begin surgically placing implants?
JG: I would take every training you can — any and every kind. University-based training is great, and I recommend going to surgical courses offered by the people offering the product so you can learn the nuances of their implant systems. I’d also suggest assisting in other dental offices where implant placement is being performed so that you can observe everything possible and learn from others. Also, just while fulfilling your required annual CE, you can lean on implant training and learn a lot. You’ve got to take the CE in any case, so you might as well learn about a field that can really help your patients and your practice while you’re at it. Even if you never decide to begin placing implants in your practice, having a better understanding of the surgical aspect can make it easier to comprehend how prosthetically driven treatment planning helps you get the best results for your patients.

Figure 1: Preoperative X-ray of tooth #30, which was diagnosed with irreversible pulpitis. Treatment options were presented to the patient, who elected for extraction, bone grafting and, after four months of healing, the placement of two implants to replace the tooth.
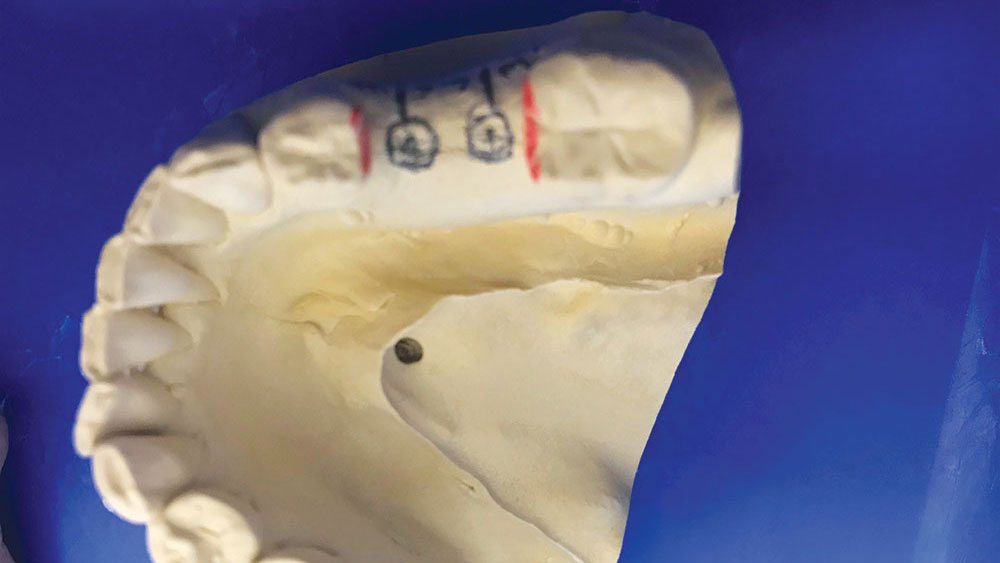
Figure 2: A diagnostic study model was used to practice the surgical procedure and obtain proper spacing and trajectory in preparation for implant placement.

Figure 3: Postoperative X-ray after placing the 3.5 mm x 11 mm Hahn Tapered Implants. Healing abutments were connected to the implants and modified temporaries were created using composite because the patient wanted something tooth-colored while the implant sites healed.

Figure 4: Four months after implant placement, lithium silicate crowns were delivered over Hahn Titanium Esthetic Abutments (Glidewell Direct). Note that the patient elected for lighter-shade implant crowns because she wants to replace the adjacent, darker restorations at a later time.
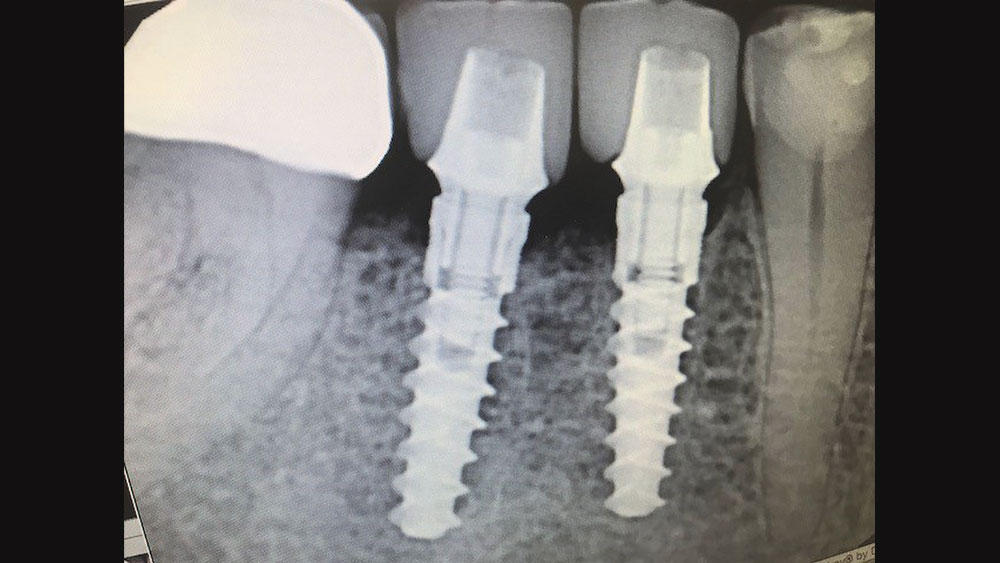
Figure 5: Four months after implant placement, lithium silicate crowns were delivered over Hahn Titanium Esthetic Abutments (Glidewell Direct). Note that the patient elected for lighter-shade implant crowns because she wants to replace the adjacent, darker restorations at a later time.
- 1
- 2
- 3
- 4
- 5