In this issue:
A Multidisciplinary Approach for the Best Esthetics
Authors



For dental professionals, having good working relationships with a variety of specialists often plays a key role in providing patients with the best treatment outcomes. The referral relationship can work in both directions, with the specialist often referring cases to the general practitioner to develop the optimal plan, particularly for complex cases.
The case below is one that came to me via Dr. Hideki Ikeda, an orthodontist I’ve worked with in the past who shares my vision of ideal treatment results. While developing his orthodontic plan of action, Dr. Ikeda recognized that restorative work would be part of the overall treatment plan, and referred the patient to me for consultation. Our successful collaboration made it possible to provide this patient the best possible outcome.
CASE ASSESSMENT: DR. IKEDA
This patient originally presented to Dr. Ikeda, asking for improvement of her anterior esthetics. Tooth #9 was impacted and tooth #10 was blocked lingually. In addition, she had an anterior open bite and crowding in both arches, and her midline was off. She also presented with a negative anterior overjet and a unique end-to-end Class II posterior occlusion.


Figures 1a, 1b: The patient originally presented to Dr. Hideki Ikeda with an impacted tooth #9, which had caused all of her other upper teeth to suffer from misalignment and crowding.
The CBCT revealed a severely impacted upper left central with a very short and dilacerated root. The prognosis of the tooth was very poor, requiring extraction.
The patient did not wish to have implant treatment, so in order to provide an upper left central, Dr. Ikeda felt that orthodontic substitution was the best option. After extraction of the impacted central, her lateral incisor (tooth #10) would be moved into the position of the missing central incisor (tooth #9). Her canine (tooth #11) would then be used to substitute as a lateral incisor, and the first premolar (tooth #12) would become the canine.
Dr. Ikeda explained that orthodontic substitution where canine teeth are used to substitute for missing lateral incisors is commonly recommended as an alternative to dental implants when patients are congenitally missing their lateral incisors. However, substituting a missing central incisor with a lateral is far less common, and presents a unique challenge in developing natural anterior esthetics.
In this case, because we were substituting the lateral incisor (tooth #10) for a missing central (tooth #9), the appearance of that tooth was more important than ever. The central incisors are the centerpiece of the smile and the key to every smile makeover. If the central incisor area does not appear natural, the patient’s entire smile will appear “off.”
With the importance of the central incisors in mind, the path was relatively straightforward. The patient’s original tooth #10, which would be moved into position #9 by Dr. Ikeda, needed to be reshaped to resemble a central incisor that matched the existing one. In addition, the other teeth being used as substitutes would also need to be adjusted to resemble the teeth they were substituting. The canine (tooth #11) needed to be modified to look like the lateral incisor (tooth #10). After that, the premolar (tooth #12) would be adjusted to look like the original canine (tooth #11).
Working closely with Dr. Ikeda, we determined not only the optimal placement for the teeth being moved, but also what specific changes to the teeth’s appearance each of us would be making and when.
The techniques typically used include interproximal reduction to adjust the width of the tooth, enameloplasty to reduce prominent cusp tips, and intrusion or extrusion to adjust the gingival position. Because of our close communication, Dr. Ikeda and I were able to bring our orthodontic and restorative skills together to plan and execute this treatment. My restorative role in treating this patient began with the process of enameloplasty. Whenever a tooth is used to substitute for one in another position, it must be reshaped and made to resemble the typical size, shape and appearance of the tooth for which it is substituting. It must also appear symmetrical to the contralateral tooth.
Once the patient agreed to the treatment plan, Dr. Ikeda bonded .018 twin brackets with the MBT™ system (3M Company; St. Paul, Minn.) on both arches. During the bonding process, the bracket placements on teeth #10–12 were adjusted to create a gingival architecture that was harmonious with the non-substitution side. Because the gingival margins of maxillary laterals are typically inferior to the centrals, the orthodontic brackets on teeth #10 and #12 were intentionally bonded more incisally to intrude the teeth and bring the gingival margins in a superior direction. Similarly, the orthodontic bracket on tooth #11 was bonded more gingivally to bring the gingival margin down.
Once tooth #10 was brought into alignment and was in the position of an upper left central, the tooth was detailed to achieve root parallelism with tooth #8. Next, open coil springs were used to create space mesial and distal to tooth #10 to match the width of tooth #9. Great care was given to the position of #10 within the space for the best possible emergence profile. At this phase, the brackets on teeth #10–12 were removed and Dr. Ikeda sent the patient back to me for temporary restorations. Dr. Ikeda also suggested that I make the incisal of tooth #10 slightly longer because more intrusion would take place later.
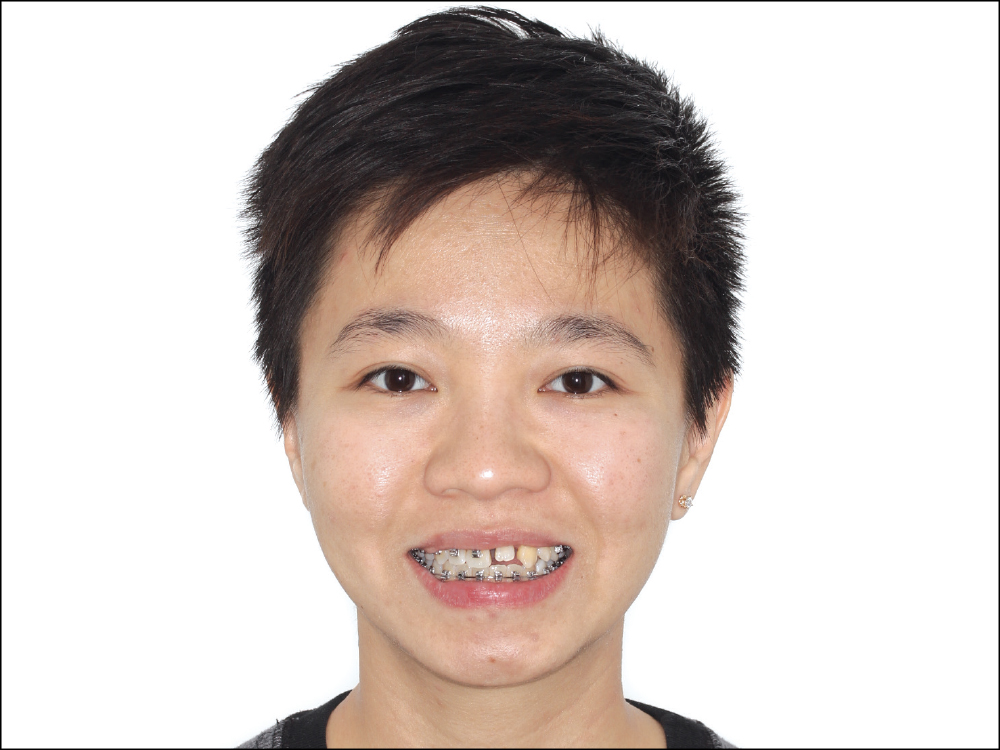
Figure 2: The patient’s presentation after Dr. Ikeda successfully moved tooth #10 into the position of #9. In this case, because we were substituting the lateral incisor (tooth #10) for a missing central (tooth #9), the appearance of that tooth was more important than ever. The central incisors are the centerpiece of the smile and the key to every smile makeover. If the central incisor area does not appear natural, the patient’s entire smile will not appear natural.

Figure 3: With the teeth positioned properly via orthodontia, enameloplasty was the next step. The goal was to reshape teeth #10–12 to match the teeth they were replacing, and to mirror the appearance of the existing teeth on the contralateral side for a symmetrical, natural-looking result.
As I began my restorative treatment, the orthodontic work Dr. Ikeda had performed was in its final stages. The brackets were still on the patient’s teeth, but most of the tooth repositioning had been completed.
My goal was now to convert the teeth to resemble as much as possible those they were replacing: I would be converting the lateral incisor to look like a central, so it could mirror tooth #8, and then would change the canine to make it look like a lateral.
In the pictures that follow, you’ll see the restorative elements of the case that transformed this patient’s smile.

Figure 4: During my first session with the patient, I used composite material to build out tooth #9 to the desired width so that it would establish the space and maintain it during the remaining orthodontic treatment prior to final crown placement. Per Dr. Ikeda’s instruction, I made the tooth longer than I typically would have so that he could intrude it to create a better gingival contour.

Figure 5: The patient returned to my office once Dr. Ikeda had successfully intruded #9 and removed all the orthodontic brackets.


Figures 6a, 6b: It was time to remove the composite material temporarily on tooth #9, and begin the process of creating final matching crowns for both #8 and #9. I removed the composite from tooth #9 and prepared it for a crown (6a), then milled and placed a provisional using BioTemps® NOW PMMA material and the glidewell.io™ In-Office Solution.

Figure 7: The importance of esthetics for the central incisors led me to select BruxZir® Esthetic Zirconia for the final restorations of teeth #8 and #9. One week after placement of the provisional, I turned back to the glidewell.io system to mill her final crowns using a BruxZir Esthetic NOW milling block.

Figure 8: I placed the final restorations, made from BruxZir Esthetic NOW in shade A1, directly after removal of the sprue. As this photo illustrates, the shade match even without any staining is incredibly close to the color of the surrounding dentition.

Figure 9: Although the shade match of the A1 blocks was already very close, and BruxZir Esthetic NOW is ready to use straight from the mill and requires no post-processing, I nonetheless chose to stain and glaze the restorations to give them more characterization and to provide an even closer match to the shade of the natural dentition.

Figure 10: The role of the central incisors as the centerpiece of the smile makes their appearance critical. Working closely with Dr. Ikeda, this patient’s natural smile was rebuilt and reshaped. She was thrilled with the final result.
CONCLUSION
Multidisciplinary cases require excellent communication between all disciplines for optimum outcomes. The unique perspective each doctor can provide based on their own background and expertise is essential in taking a case’s outcome to the next level. In the case previously detailed, coordination between Dr. Ikeda and me allowed us to evaluate the positioning of each of the teeth being moved, which in turn let us confirm that we were working toward a shared vision of success.
Excellent working relationships such as this one, with seamless communication and coordination, make treating a case more enjoyable and gratifying. Even more importantly, it benefits the patient, who enjoys the expertise of more than one skilled doctor working to achieve the best possible result.
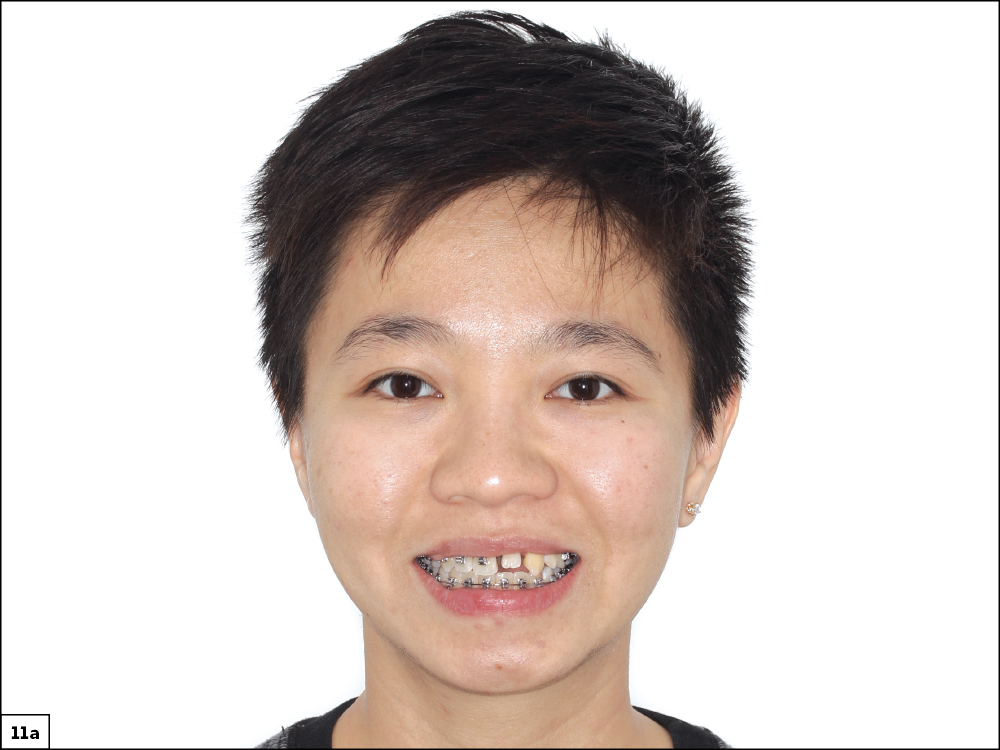

Figures 11a, 11b: A before-and-after comparison of the patient’s smile shows the extensive improvements that took place through our multidisciplinary collaboration. She will enjoy this new look as she moves forward in her life with renewed confidence.