
In this issue:
The Half-Arch Restoration: Solving a Challenging Problem with a Solid Zirconia, Implant-Supported Prosthesis
Author
The chief complaint from my patient, Weldon, was missing teeth and gaps between his teeth. The preoperative evaluation showed periodontally involved and non-restorable maxillary right teeth #2–8 and significant periodontal bone loss, which would need to be addressed. The periodontal condition was stable in the patient’s left maxilla, and he was satisfied with the existing esthetics in that quadrant.
Restoring function to half an arch can be challenging, and our options included the following:
- Removal of the maxillary right teeth and fabrication of a partial denture
- Removal of the maxillary right teeth, dental implant treatment and one of the following:
- A removable, implant-supported, unilateral palateless overdenture, retained with either individual attachments or a bar and clip-type system
- A screw-retained hybrid appliance, which would compensate for tissue loss with the use of gingival-colored, layered material in the apical portion of the restoration
- A fixed, all-zirconia implant-supported prosthesis with pink gingival areas, which would provide both long-term durability and ideal esthetics
Weldon desired “permanent teeth” and rejected the option of a removable appliance, as he was dissatisfied with the partial he had been wearing prior to treatment. As a 70-year-old with controlled hypertension, no other significant medical considerations, and relatively healthy, functional and esthetic maxillary left teeth, he elected to restore the maxillary right quadrant with a fixed, implant-supported prosthesis. BruxZir® Solid Zirconia is my material of choice for this type of restoration because of its strength and esthetics. Further, the material can be milled as a monolithic implant bridge, with lifelike pink stain applied to the gingival areas, to predictably and fully restore form and function for the patient, even in edentulous spans where significant tissue loss has occurred.
BruxZir Solid Zirconia is my material of choice for this type of restoration because of its strength and esthetics.
INITIAL PHASE OF TREATMENT
The process of restoring Weldon’s teeth began by determining what the final prosthesis would look like. Glidewell Laboratories has a proven protocol that helps dentists address any prosthetic considerations during the initial phase of treatment planning. The lab evaluated the case prior to the surgical intervention and made suggestions for developing the ideal final prosthesis. It’s helpful to illustrate to the patient what the end result will be, especially in a situation like this, where there was significant unilateral vertical bone loss. It is important that the patient understands the concept of a prosthesis that includes pink gingival areas. We cannot assume our patients will understand the final result.
The Hahn™ Tapered Implant (Glidewell Direct; Irvine, Calif.) was ideal for this case because it has a pronounced thread design, a machined collar for soft-tissue maintenance, and a prosthetic connection that facilitates platform switching, which serves to preserve bone and gingival tissue around the implant-abutment interface.
SURGICAL CONSIDERATIONS
Bone Loss
There was significant bone loss on the right side of the maxilla, from the existing non-restorable central incisor back to the second molar. With this bone loss and mobility of the teeth, there was vertical and horizontal deficiency of the available bone. Options considered included an autogenous block graft to attempt to increase bone height and width. The second option was to work with the available bone, extract the non-restorable teeth on the right side of the maxillary arch, immediately place implants, and create esthetics with a longer prosthesis that includes pink-colored gingival areas. A BruxZir Solid Zirconia implant bridge was the optimal long-term solution because the entire prosthesis, including the gingival areas, is milled from a single block of high-strength solid zirconia, affording unmatched durability for this type of restoration. Although Weldon did not have a high smile line, he was attracted to a prosthetic design that included gingival areas to restore esthetics where tissue loss had occurred.
“I chose to receive implants because I got tired of taking my partial out and putting it in a jar at night. ... I’m very happy. Everywhere I go, I’ve had nothing but compliments.”
–Weldon R.
Ideal Implant Selection and Grafting of the Site
The Hahn™ Tapered Implant was chosen for Weldon because it is ideally suited for this type of case. For example, the pronounced threads excel in establishing initial implant stability in a fresh socket site. The machined collar helps to prevent bone loss around the neck of the implant and also has a cleansable surface. The prosthetic connection with built-in platform-switching helps to minimize the resorption that could occur with other systems, where the connection between the implant and abutment is at bone level, by preventing a microgap and potential bacterial invagination. And of course, the Hahn Tapered Implant System allows for either a cemented or screw-retained restoration.
After removing the untreatable teeth, I placed five Hahn Tapered Implants into the extraction sockets, grafted the area with Newport Biologics™ Mineralized Cortico/Cancellous Allograft Blend (Glidewell Direct) mixed with harvested autograft from the osteotomy sites, and used a Newport Biologics Resorbable Collagen Membrane 3-4 (Glidewell Direct) as a barrier against epithelial downgrowth during the healing and remodeling phase.
RESTORING THE CASE
Following integration of the implants for approximately four months, a final impression was made using Hahn Open-Tray Impression Copings (Glidewell Direct). The laboratory created a master cast and fabricated Inclusive® Titanium Custom Abutments for a cementable, implant-supported prosthesis. A screw-retained prosthesis was considered for this case, but because of the angulation of the seated implant fixtures, access holes would have exited through the facial aspect of the final prosthesis. Note that the patient is able to maintain the health of the tissue in the area of the restoration with a water pick, and the BruxZir Solid Zirconia material resists bacterial adhesion.
RESTORATIVE TECHNIQUES FOR ESTHETICS AND OCCLUSION
Esthetics and occlusion can be challenging in these types of cases. Restoring half an arch and trying to mirror the contralateral soft tissue and dentition with proper contours and shade requires patience and resolve. The lab provided a PMMA try-in prosthesis, which I evaluated with Weldon. The try-in allowed us to easily resolve any discrepancies with the prosthetic design and develop ideal occlusion. Once Weldon agreed on the esthetics, the PMMA provisional was returned to the lab and duplicated in BruxZir Solid Zirconia. This extra step eliminates excessive chairside adjustments upon seating of the final prosthesis.

Figure 1: Preoperative and retracted view of the periodontally involved and non-restorable maxillary right teeth #2–8.
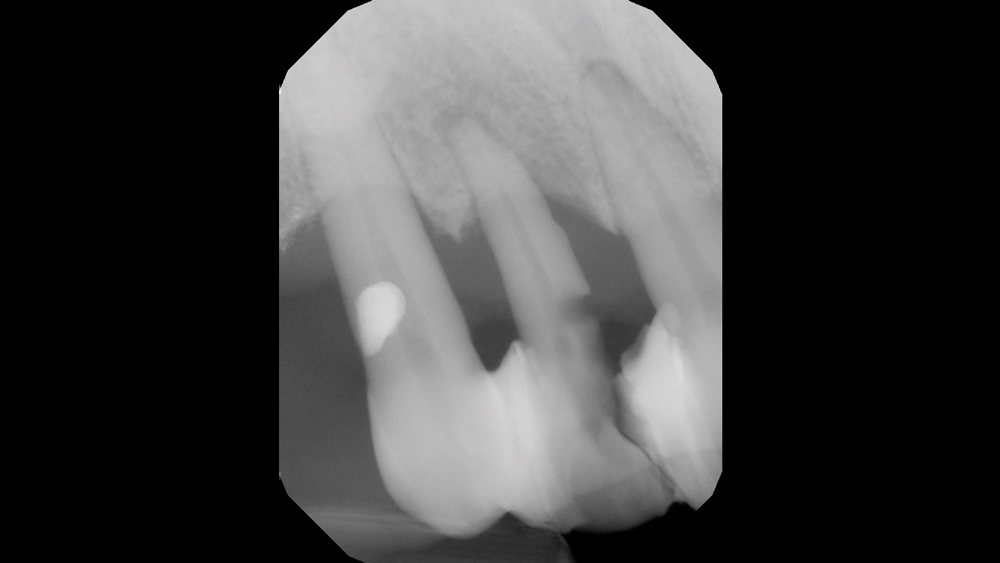
Figures 2a, 2b: Preoperative radiography confirmed that the mobile teeth needed to be removed.
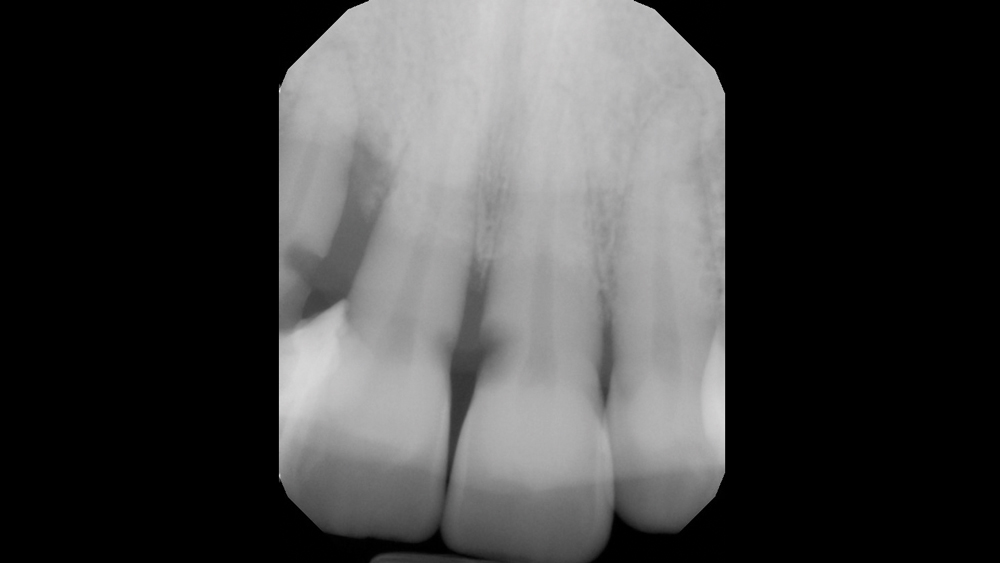
Figures 2a, 2b: Preoperative radiography confirmed that the mobile teeth needed to be removed.
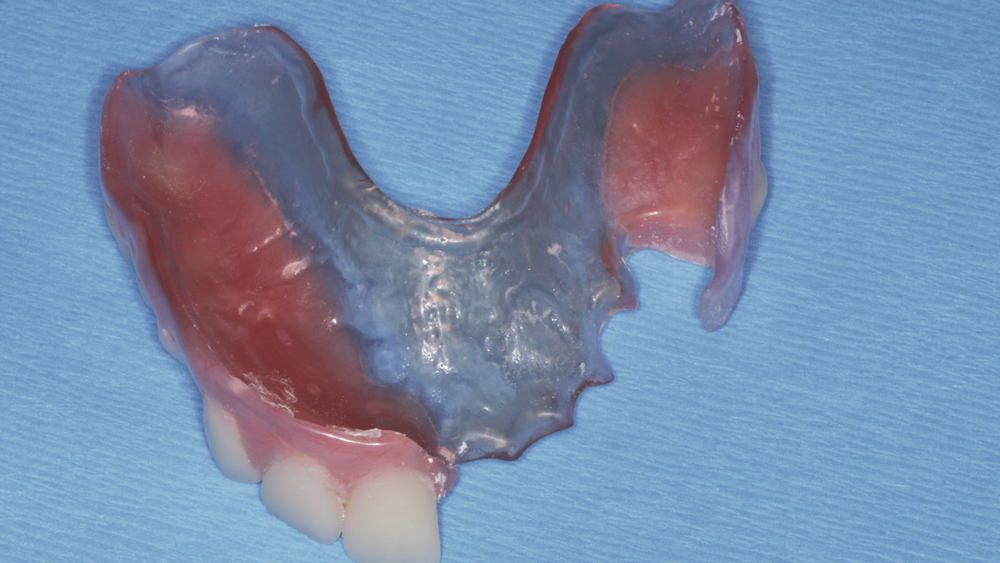
Figure 3: The laboratory fabricated a removable appliance to be seated following extraction and implant placement for use during the period of osseointegration.
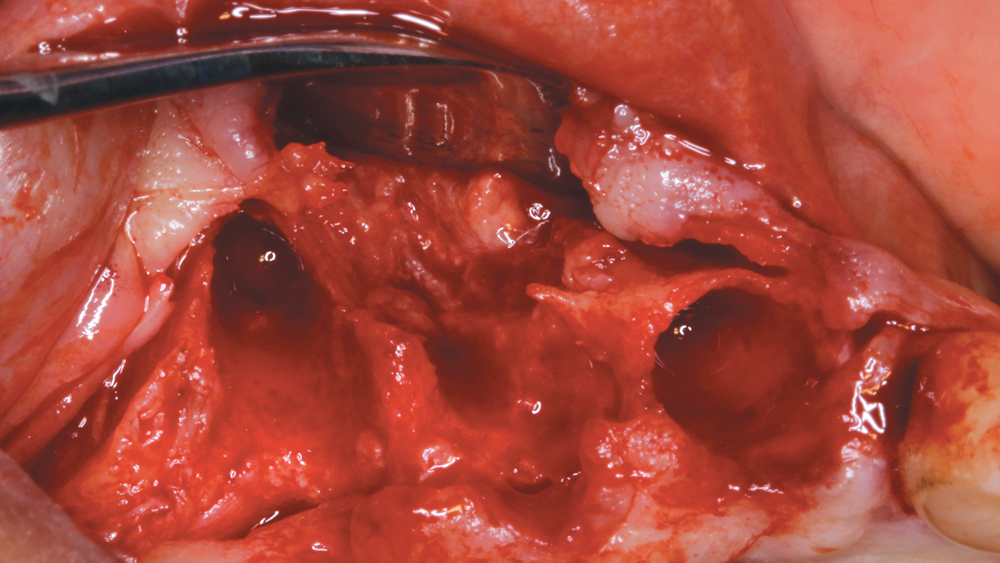
Figure 4: The teeth were removed, and the soft tissue was reflected to expose the defective bone contours prior to implant placement.
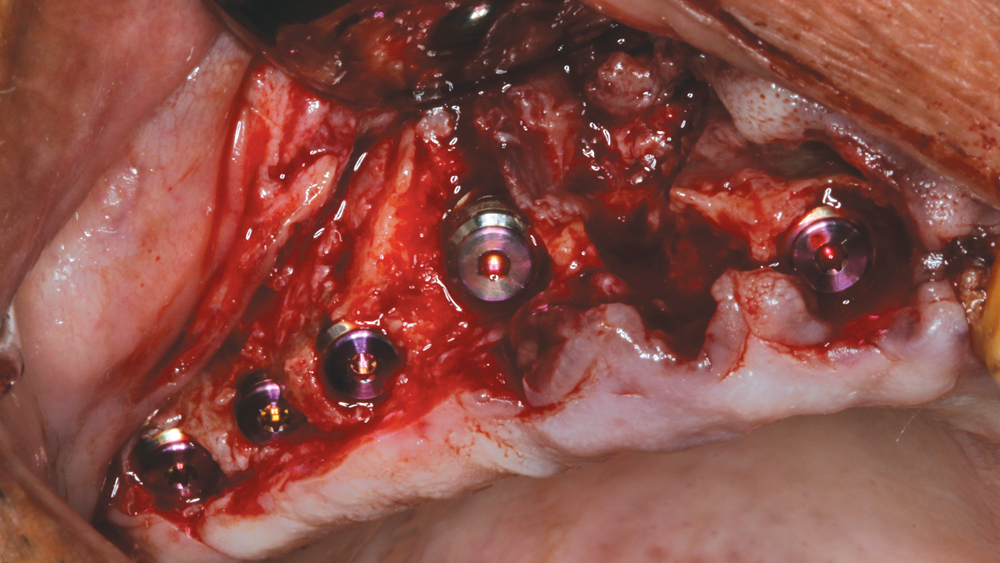
Figure 5: Five Hahn Tapered Implants were immediately placed into the socket sites using the Hahn surgical protocol.
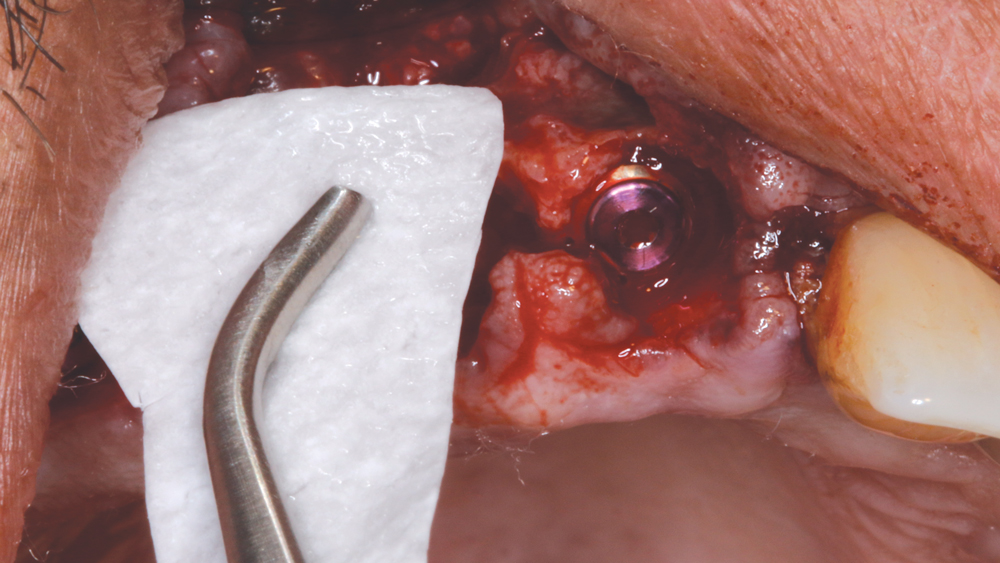
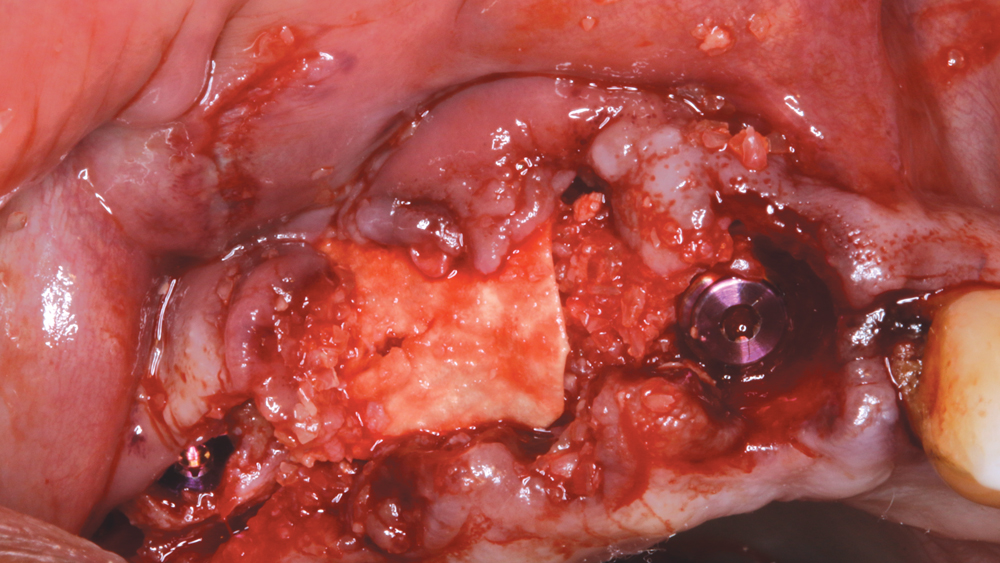
Figure 6: A Newport Biologics Resorbable Collagen Membrane 3-4 was cut to size to extend beyond the defect, which would be corrected with allograft material. The membrane prevents invagination of epithelial tissue into the healing wound.
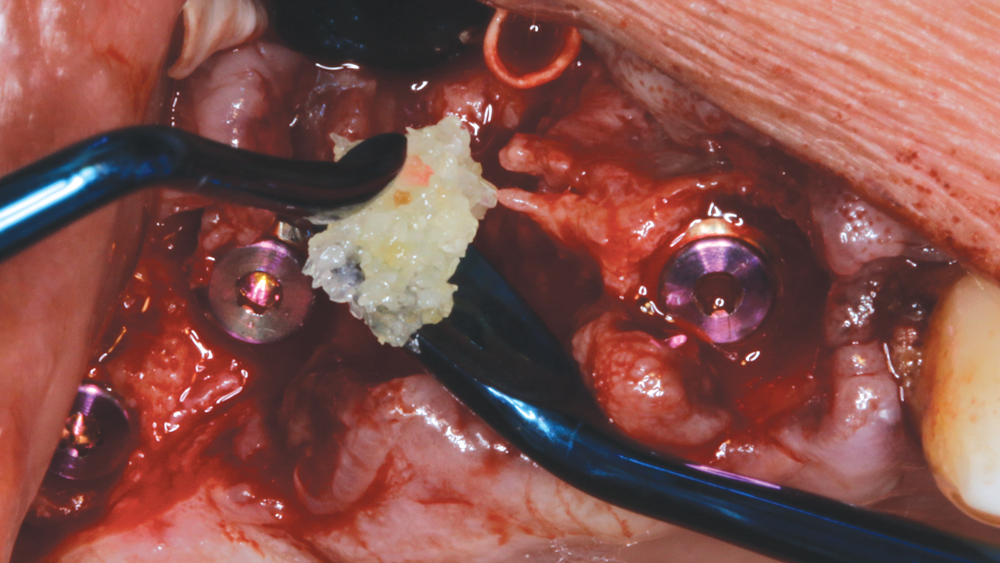
Figures 7a, 7b: Newport Biologics Cortico/Cancellous Allograft Blend was placed firmly but carefully, and the membrane was passively tucked facially and palatally.
Figures 7a, 7b: Newport Biologics Cortico/Cancellous Allograft Blend was placed firmly but carefully, and the membrane was passively tucked facially and palatally.
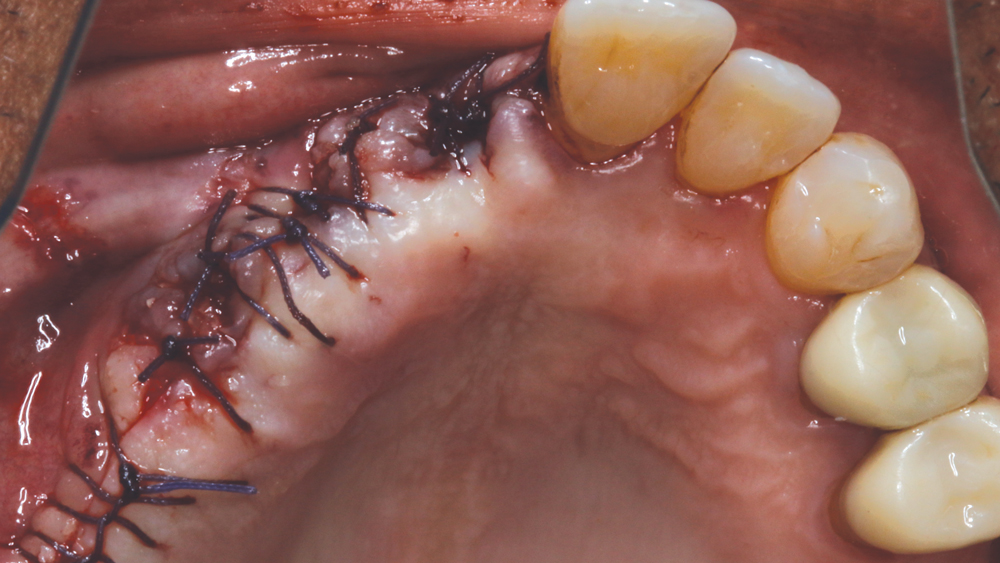
Figure 8: VICRYL™ suture (Ethicon; Somerville, N.J.) was used to close the reflected gingival tissue.
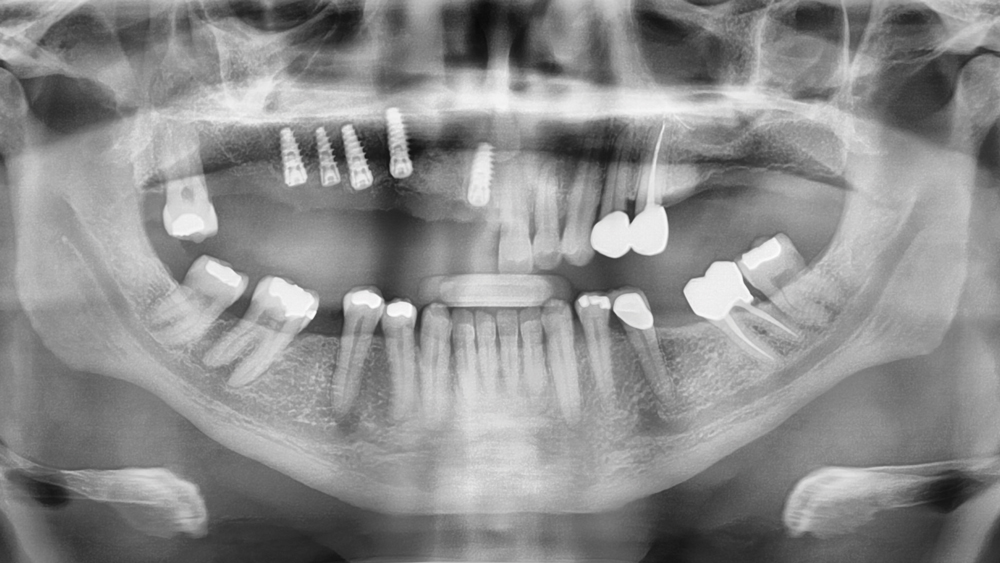
Figure 9: Postoperative panoramic radiograph illustrates the positioning of the Hahn Tapered Implants in the maxillary right quadrant.

Figure 10: After a few weeks of healing, the tissue had responded well and was pink, firm and healthy.

Figures 11a, 11b: Inclusive Custom Abutments were fabricated with gingival or slightly subgingival margins. The abutments were delivered using lab-created seating jigs to ensure proper orientation, and the prosthetic screws were tightened to 35 Ncm. Proper torque is critical to preventing abutment loosening over time.

Figures 11a, 11b: Inclusive Custom Abutments were fabricated with gingival or slightly subgingival margins. The abutments were delivered using lab-created seating jigs to ensure proper orientation, and the prosthetic screws were tightened to 35 Ncm. Proper torque is critical to preventing abutment loosening over time.

Figures 12a, 12b: The PMMA try-in prosthesis was created by the lab to help fine-tune the contours and occlusion. This allowed any necessary adjustments to easily be made to the prosthetic design prior to milling the final BruxZir restoration. The patient was also involved in making any esthetic changes to the try-in prosthesis.

Figures 12a, 12b: The PMMA try-in prosthesis was created by the lab to help fine-tune the contours and occlusion. This allowed any necessary adjustments to easily be made to the prosthetic design prior to milling the final BruxZir restoration. The patient was also involved in making any esthetic changes to the try-in prosthesis.

Figures 13a, 13b: Because of the excessive vertical bone loss created by the periodontally involved teeth, it was determined that the final BruxZir Solid Zirconia prosthesis would be designed and milled with gingival areas and pink coloring to maximize esthetics. A gingival shade guide was used to select the proper shade for the soft-tissue portion of the prosthesis.

Figures 13a, 13b: Because of the excessive vertical bone loss created by the periodontally involved teeth, it was determined that the final BruxZir Solid Zirconia prosthesis would be designed and milled with gingival areas and pink coloring to maximize esthetics. A gingival shade guide was used to select the proper shade for the soft-tissue portion of the prosthesis.

Figures 14a–14c: The final BruxZir Solid Zirconia prosthesis was seated and evaluated.

Figures 14a–14c: The final BruxZir Solid Zirconia prosthesis was seated and evaluated.

Figures 14a–14c: The final BruxZir Solid Zirconia prosthesis was seated and evaluated.

Figures 15a, 15b: The desired smile design was achieved, and the patient was thrilled with the functional and esthetic final result.

Figures 15a, 15b: The desired smile design was achieved, and the patient was thrilled with the functional and esthetic final result.
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
The PMMA try-in prosthesis ... allowed any necessary adjustments to easily be made to the prosthetic design prior to milling the final BruxZir restoration.
BruxZir Solid Zirconia has proven to be extremely strong yet compatible with opposing natural dentition; the material exhibits minimal wear on the opposing enamel. Its color and shading are extremely natural in appearance, and I have no concerns about chipping or cracking of the material over time. The final seating of the prosthesis was straightforward, and I have confidence that the material is a long-lasting solution. Weldon was thrilled with the final restoration, as we were able to surpass his expectations and provide him with a fixed, functional, esthetic result.
CONCLUSION
Ten years ago, 75 percent of my surgeries were done under intravenous sedation. Today, the surgical procedure is routine, and implant dentistry has become an accepted and predictable means of replacing missing or diseased teeth. The process has been simplified, and the prosthetic materials and surgical protocol have allowed practitioners to improve the quality of our patients’ lives.
Understanding the foundation required to predictably place dental implants, including effective extraction techniques, socket management and grafting procedures, has improved the prognosis. Working with talented and well-trained laboratory technicians helps us plan the final prosthetic result prior to any surgical procedure. Innovative laboratory techniques and materials provide outstanding functional and esthetic results. As for Weldon, his BruxZir implant bridge ensures an excellent long-term prognosis as well as restored esthetics in an area that was compromised by tissue loss prior to treatment.