In this issue:
Implant Bar Overdentures
Author

Dr. Stephanie Tilley’s patient featured in the case report of this article.
Note: The Hahn Tapered Implant System is now known as the Glidewell HT Implant System
For more than 30 years, dental implants have been the preferred mode of treatment for the edentulous arch because of the improved function and esthetics that patients enjoy.1 2 The fixed full-arch restoration, such as the BruxZir® Implant Prosthesis, is considered the premium option for our edentulous patients, but, unfortunately, not every patient is a candidate. This restorative option is limited to patients who have sufficient quantity and quality of bone to receive at least four implants and to establish an adequate anterior-posterior (A-P) spread. In addition, the cost of fixed implant restorations is out of reach for many edentulous patients and some patients are unable to maintain adequate hygiene around a fixed restoration.
The implant overdenture remains an excellent alternative for patients who cannot receive a fixed restoration due to financial considerations, anatomical deficiencies or the inability to maintain oral hygiene.
The design of implant overdentures can be divided into two general categories: (1) freestanding implants; and (2) implants connected with a cast or milled bar. With freestanding implants, two or more implants are fitted with retentive attachments, such as the Locator® (Zest Anchors; Escondido, Calif.), which attach to a matching retentive device in the denture base. This type of overdenture is considered implant-retained, but it is supported by the patient’s soft and hard tissues.
By contrast, in a bar overdenture, the attachments are an integral part of a bar, which connects the implants together. Because this design better distributes functional forces among the implants connected to the bar, the prosthesis can be partly implant-supported and requires less support from the patient’s own tissues.
The implant overdenture remains an excellent alternative for patients who cannot receive a fixed restoration due to financial considerations, anatomical deficiencies or the inability to maintain oral hygiene.
CASE REPORT
This patient had been edentulous for several decades when she presented for treatment, requesting a more stable mandibular denture. We provided the patient with a Locator CAD/CAM-Milled Bar Overdenture (Glidewell; Newport Beach, Calif.), which includes Locator attachments integral to the bar. The implant bar overdenture helped maximize prosthetic support and retention for the patient despite her anatomical deficiencies. The restoration also helped the patient avoid the time and expense of the additional surgical procedures that would have been necessary for a fixed full-arch implant restoration, which was not within the patient’s budget.
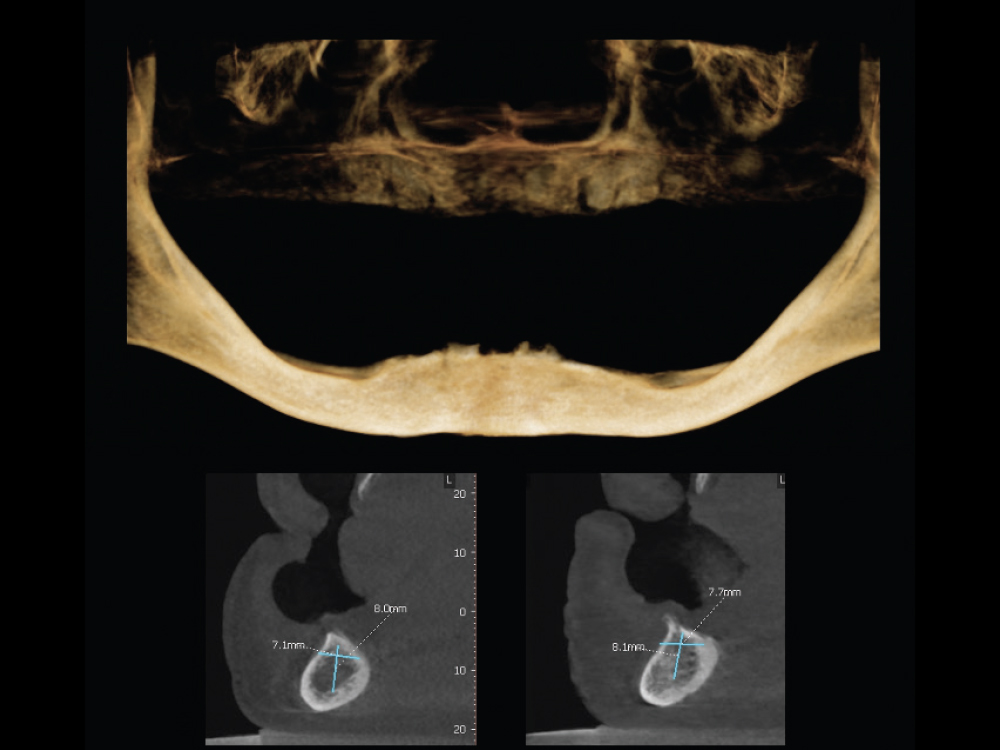
Figure 1: The patient requested implant treatment for her edentulous mandible, as her existing complete denture was loose-fitting and unstable. The sagittal view of the CBCT scan shows sufficient bone for implant placement in the symphysis area, while the posterior areas would require extensive bone grafting to allow for implant placement. The patient accepted a treatment plan in which two implants would be placed in the anterior to support an implant overdenture. Because the anatomical deficiencies of the patient’s mandible required positioning of the implants in the anterior, a bar would be used to situate the Locator Abutments further toward the posterior, providing for increased stability of the overdenture.
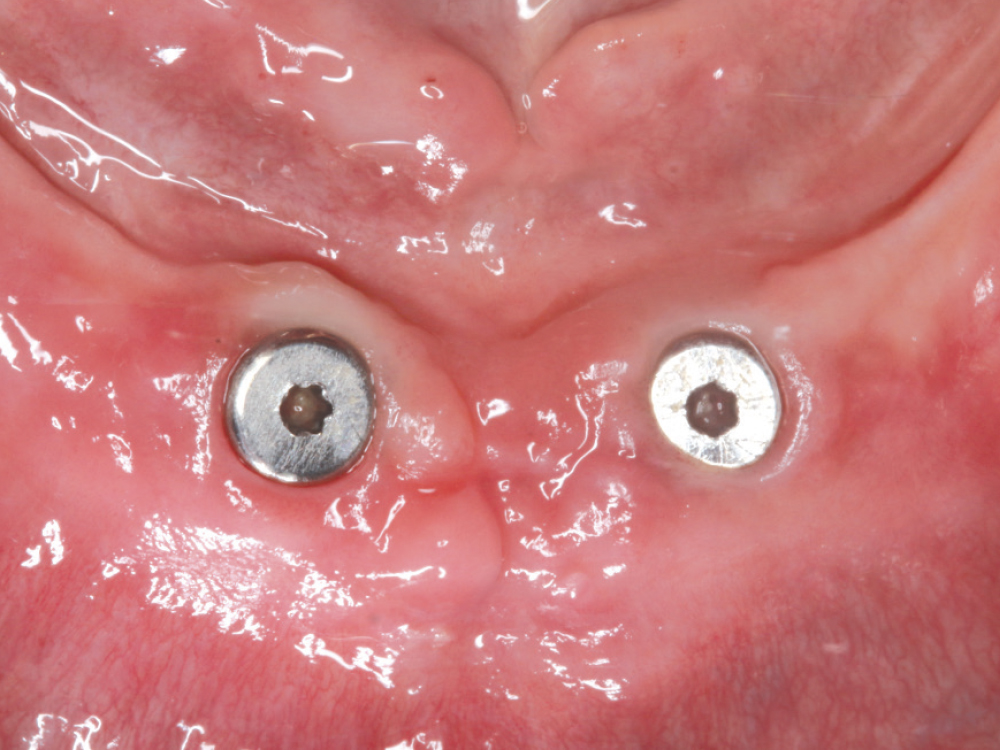
Figure 2: At the surgical appointment, a flap was reflected and two 3.5 mm x 8 mm Hahn™ Tapered Implants (Glidewell Direct; Irvine, Calif.) were placed in the anterior. Because the implants achieved insertion torque of 40 Ncm, 3-mm-tall healing abutments were connected to the implants, allowing for some stability of the patient’s existing complete denture and avoiding a second surgery for implant uncovering. The patient returned three months later for evaluation.

Figure 3: With the implants fully integrated and good soft-tissue health evident at the implant sites, the healing abutments were removed and an open-tray impression was taken using a custom tray provided by Glidewell. This allowed for a very accurate final impression of the residual ridge.
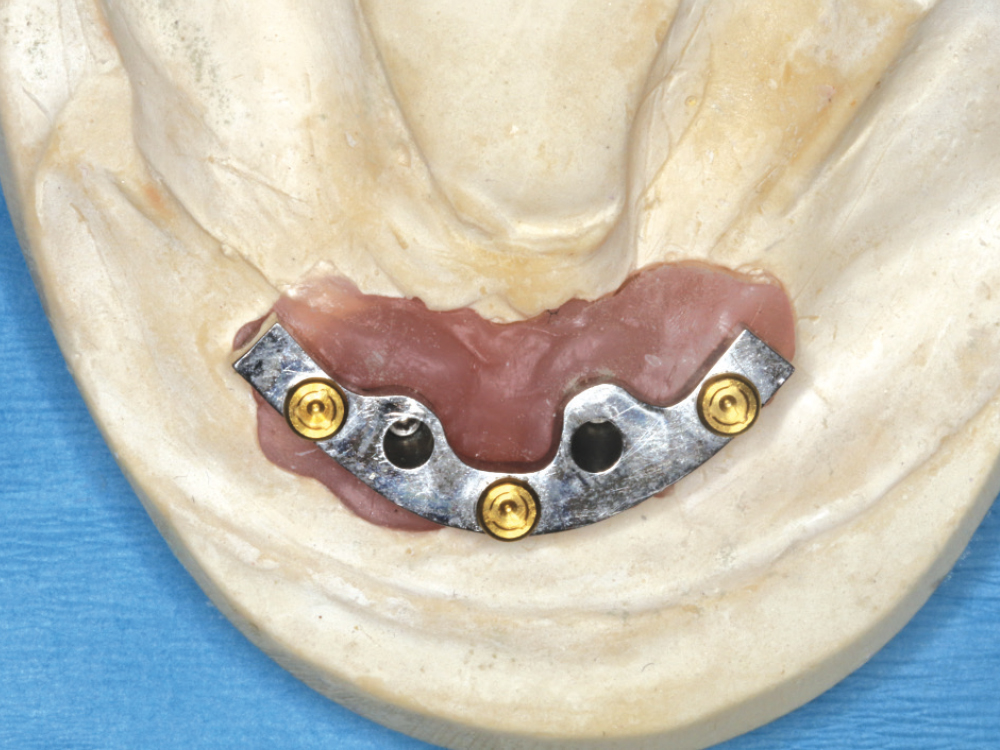
Figure 4: Due to the lack of posterior bone volume, the implants were placed in close proximity in the symphysis area of the mandible. Glidewell designed and fabricated a milled titanium bar connecting the two implants. This allowed for the placement of three Locator attachments on the bar, resulting in a retentive and significantly more stable denture. The implant bar would also take pressure off the bone and soft tissue in the anterior, resulting in a prosthesis that is tissue-supported only in the posterior.

Figure 5: A conventional denture fabrication protocol was completed, with wax rims adjusted to establish the occlusal plane and the vertical dimension of occlusion. Denture teeth were set in wax, tried in, and evaluated for occlusion, esthetics, shade, tooth arrangement and midline. Once the patient approved the wax setup, the Locator CAD/CAMMilled Bar Overdenture was processed by Glidewell.

Figure 6: The CAD/CAM-milled Locator bar was connected to the implants and torqued into place at 25 Ncm. Note how the bar elevates the prosthetic connections, minimizing pressure on the bone and soft tissue in the area of the implants.
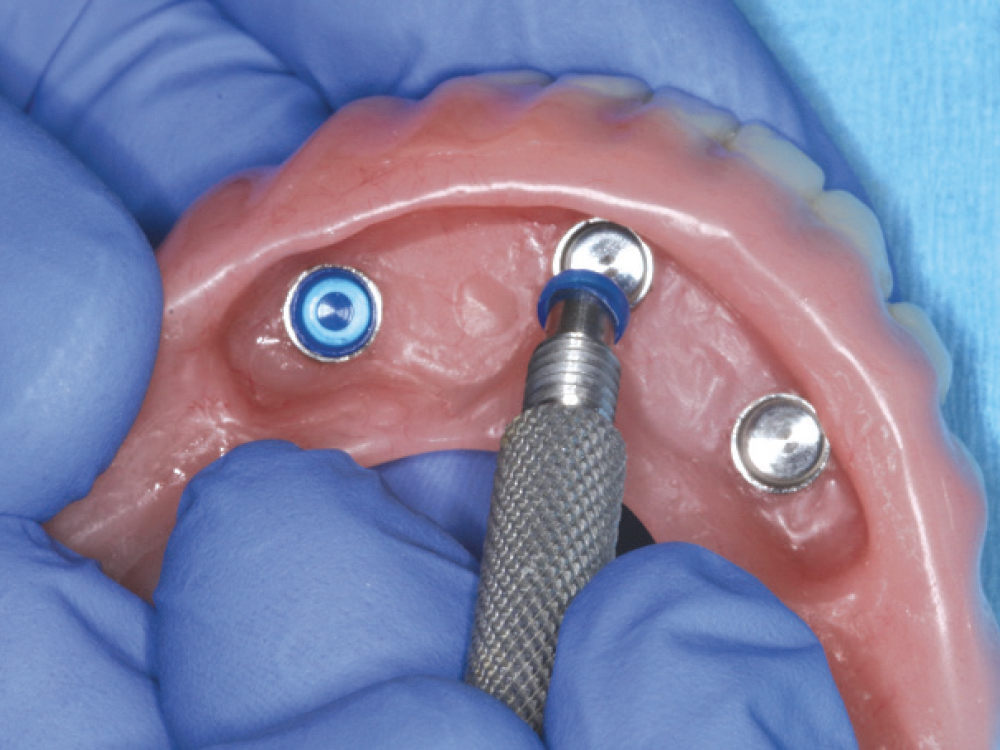
Figure 7: Before delivering the overdenture, the black processing caps were removed and replaced with blue retentive caps, which seat within Locator housings that are cured into the overdenture during lab fabrication. The housings and nylon caps serve to retain and stabilize the denture when seated over the Locator Abutments on the implant bar. The nylon caps come in a number of retentive strengths and are easily replaced when wear occurs over time or if the patient requests greater retention. According to the manufacturer, the retentive caps resist wear during up to 56,000 cycles of function.

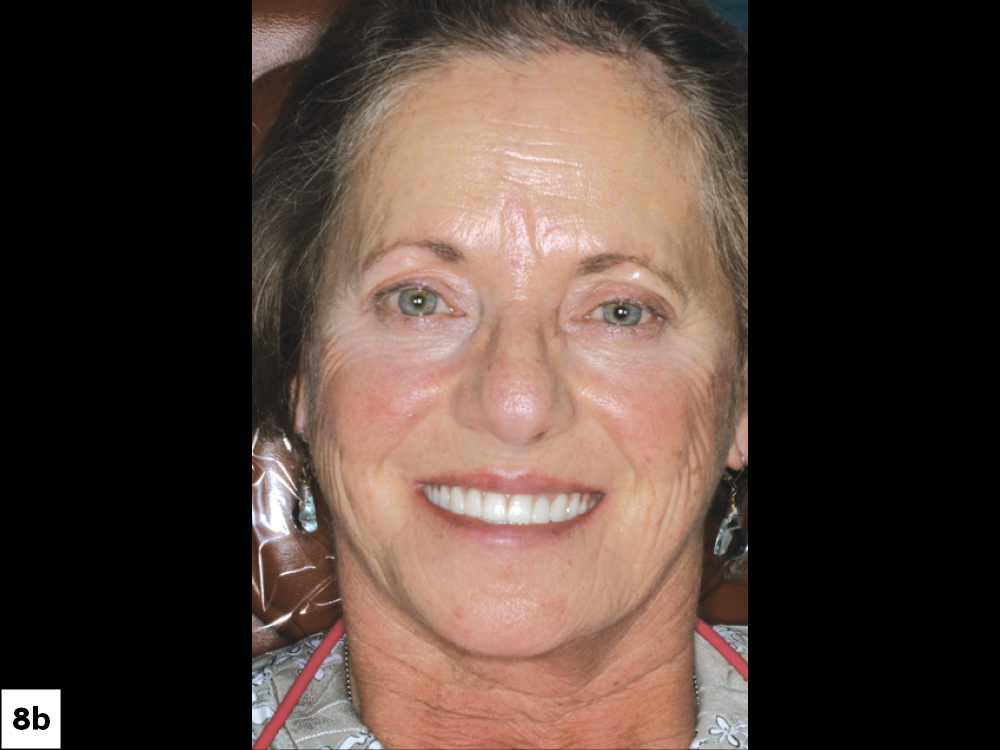
Figures 8a, 8b: The final implant-retained mandibular overdenture was snapped into place, creating excellent form and function. The overdenture exhibited excellent stability, including very little anterior-posterior rocking.
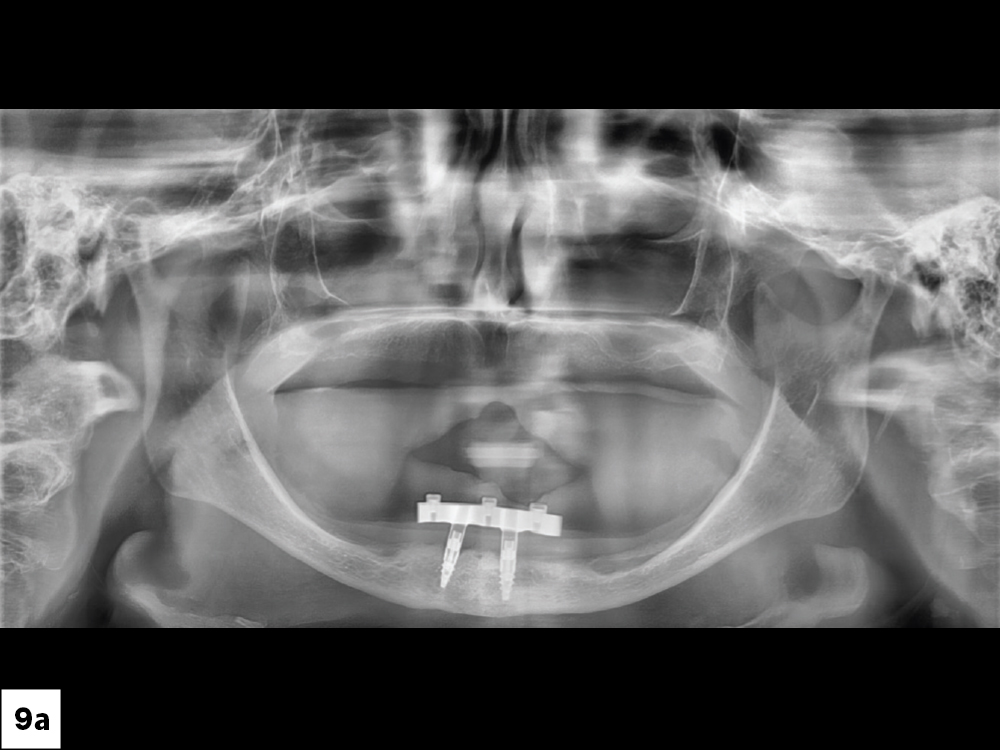
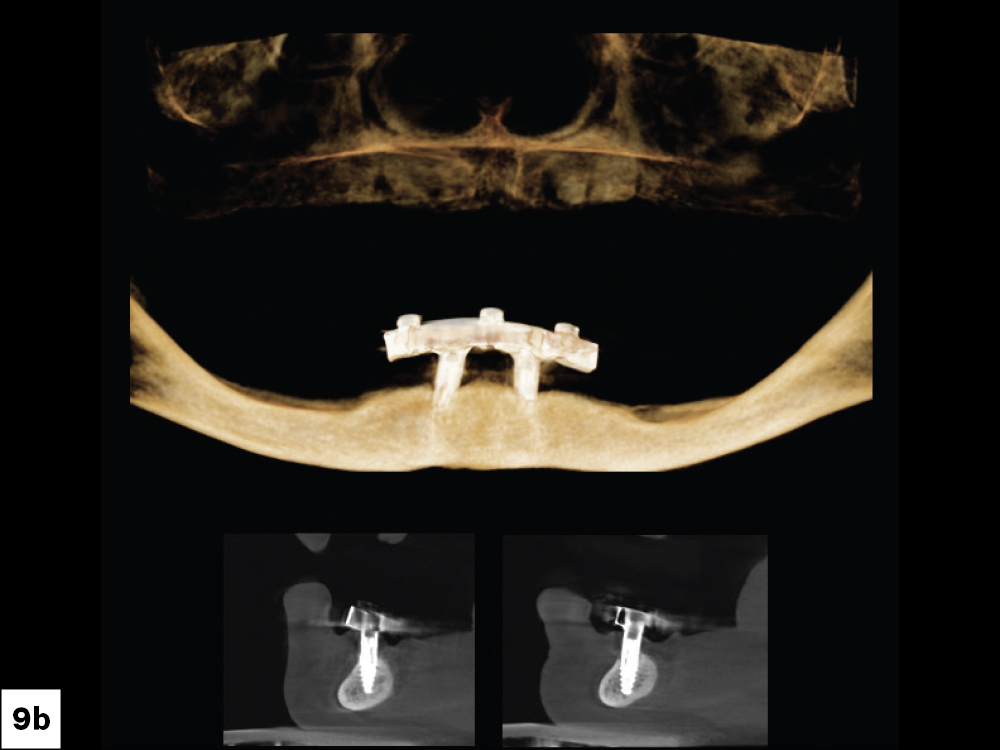
Figures 9a, 9b: The final panoramic radiograph and CBCT imaging captured at the final delivery appointment for the overdenture.

Figure 10: The occlusion was evaluated, and the patient was instructed on insertion, removal and home care of the implant overdenture.

Figure 11: The patient was extremely happy with her final mandibular overdenture, which is far more stable than her previous denture and has substantially increased her chewing ability.
CONCLUSION
Treatment with an implant bar overdenture resulted in significant improvement in quality of life for this patient. Implant overdentures provide excellent esthetics and function for many patients and help address budget limitations. Providing this type of care is rewarding to me professionally and greatly appreciated by my patients. Understanding the array of prosthetic options available for the fully edentulous arch allows us to find the optimal solution for individual patients depending on their specific needs.
References
- ^ Yunus N, Masood M, Saub R, Al-Hashedi AA, Taiyeb Ali TB, Thomason JM. Impact of mandibular implant prostheses on the oral health-related quality of life in partially and completely edentulous patients. Clin Oral Implants Res. 2016 Jul;27(7):904-9.
- ^ Martín-Ares M, Barona-Dorado C, Guisado-Moya B, Martínez-Rodríguez N, Cortés-Bretón-Brinkmann J, Martínez-González JM. Prosthetic hygiene and functional efficacy in completely edentulous patients: satisfaction and quality of life during a 5-year follow-up. Clin Oral Implants Res. 2016 Dec;27(12):1500-5.