
In this issue:
A Review of Implant-Retained Overdentures
Authors
Despite the popularity of fixed full-arched restorations, implant overdentures remain a valid treatment option for many patients. Considerations include:
- Cost: Implant-retained overdentures can usually be provided at a significantly reduced cost compared to fixed restorations. In many cases, a patient’s existing complete denture can be retrofitted to the newly placed implants, reducing costs even further.
- Insufficient Bone Volume: Some patients might not have enough bone volume for an adequate number of correctly positioned implants to provide the appropriate support for a fixed restoration. Instead, they may be eligible for an overdenture, which requires a minimum of two implants in some cases.
- Grafting Contraindicated: In many cases, bone grafting is needed to facilitate the placement of the implants for a fixed full-arch prosthesis. If patients are unable to receive bone grafting due to health or financial reasons, overdentures should be discussed.
- Patient Preference: Some patients are content with their conventional removable appliances but simply want more retention. Overdentures offer the esthetics of traditional dentures with better retention.
CASE REPORT NO. 1
Freestanding Locator Attachments




Overdentures offer the esthetics of traditional dentures with better retention.







 impression material")





















CASE REPORT NO. 2
Bar-splinted Mandibular Case





CASE REPORT NO. 3
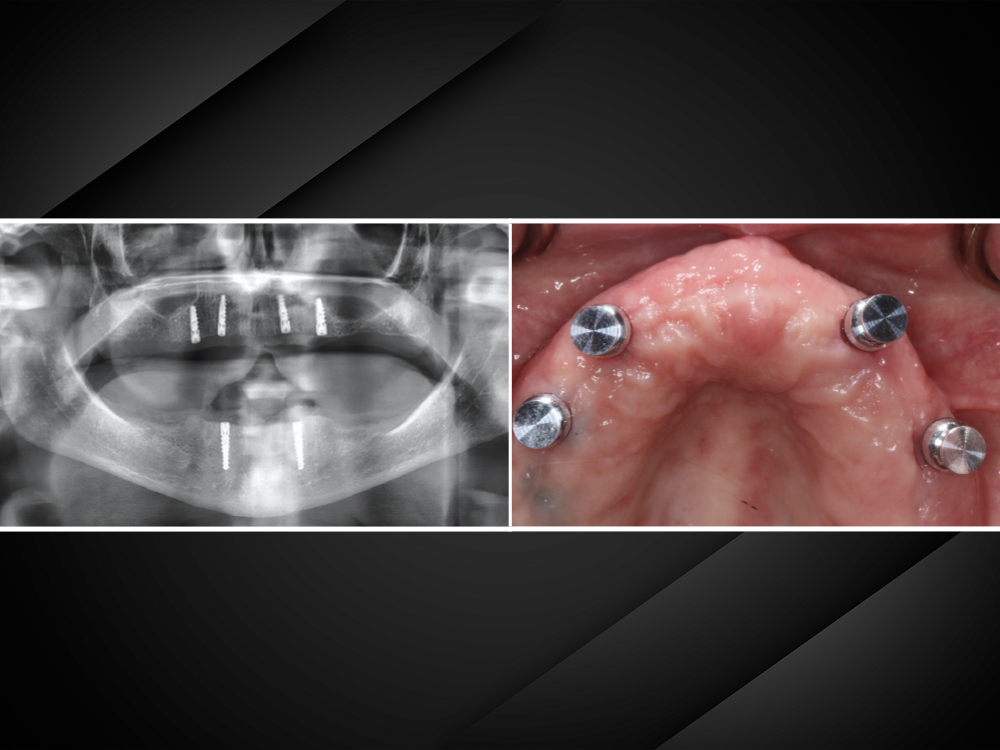
Maxillary Case with Intraoral Pickup and Chairside Processing of Locator Housings









CONCLUSION
When determining the best treatment plan for an edentulous patient, their health, available bone structure and budget are the most important factors. Implant-retained overdentures can greatly improve a patient’s quality of life. To ensure success, it’s crucial to have open communication with patients about which procedures are feasible, predictable and affordable.
VOCO is a registered trademark of VOCO America, Inc.