
In this issue:
Implant Impressions: The Digital Approach for the Single Unit (1 CEU)
Author

Capturing an accurate impression is an essential part of dentistry, particularly when restoring a rigid, osseointegrated implant. Inaccurate capture of the implant position can lead to an ill-fitting prosthesis, which could result in undesirable complications. In my experience, the accuracy and detail obtained with digital impressions provide a clear advantage over conventional impressions. Not only is intraoral scanning more comfortable for patients, it also allows doctors to instantly send digital impressions to the lab. Because scans can be uploaded and stored electronically, they enable doctors to easily check for distortions, analyze margins and confirm accuracy — all while the patient is still in the chair. This article details the best practices for taking digital impressions of single-unit implant cases.
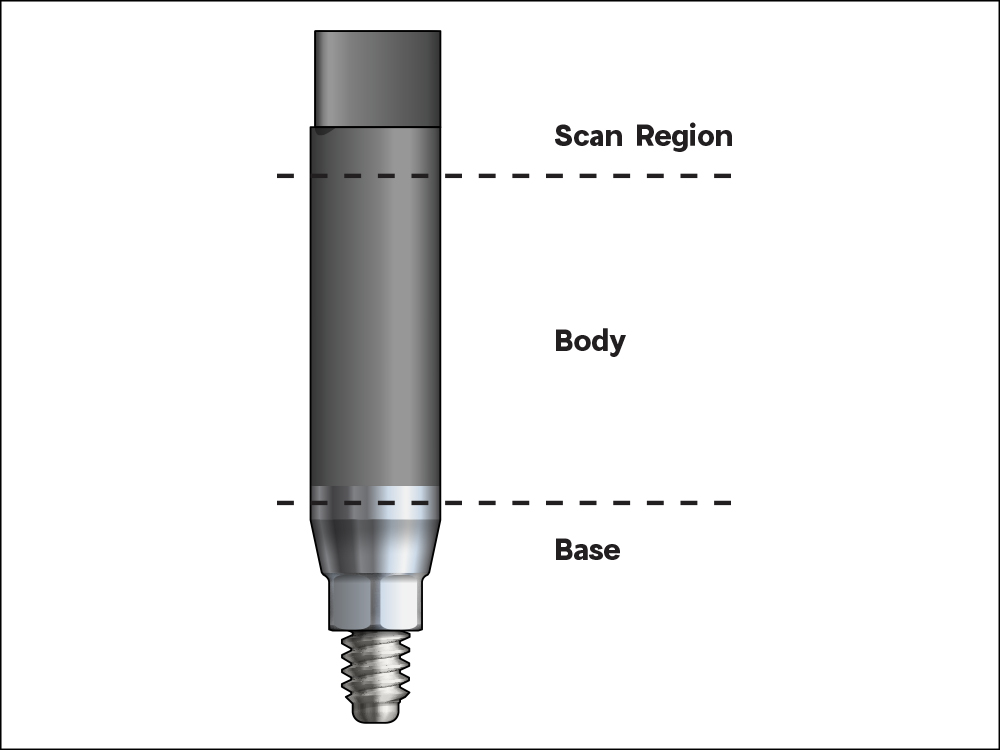
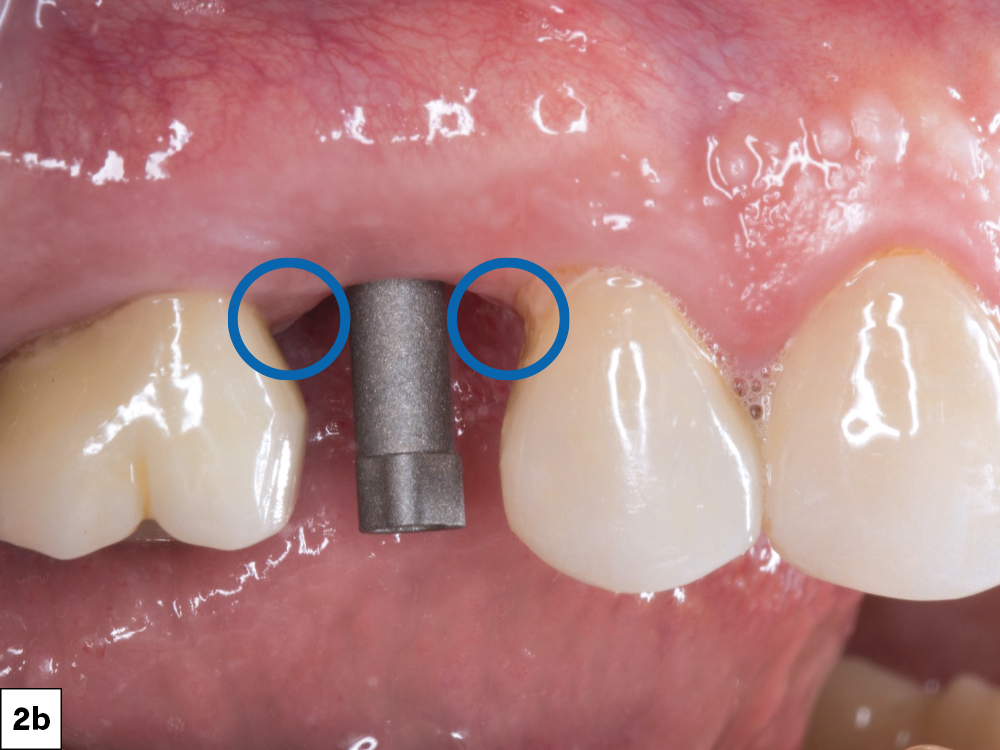
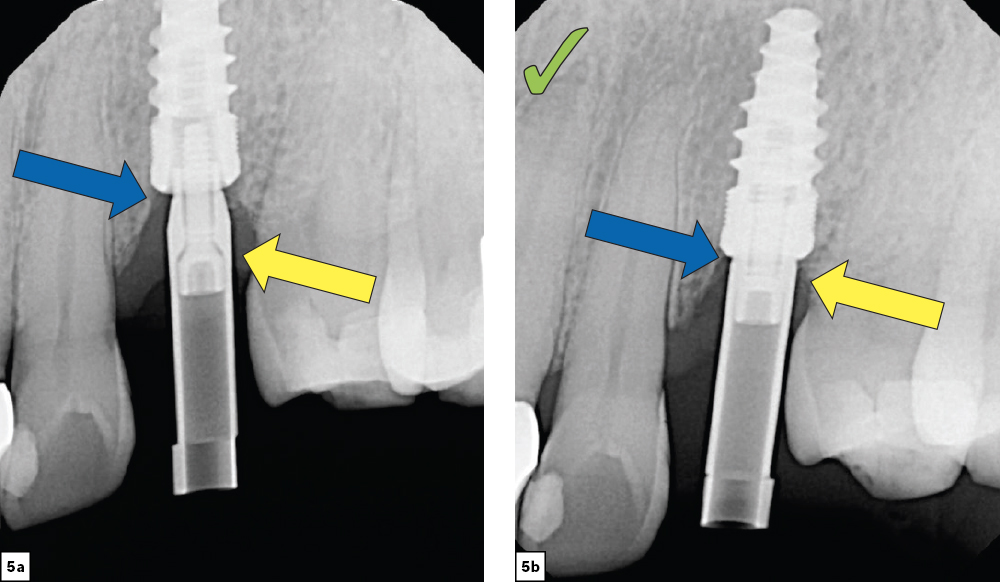
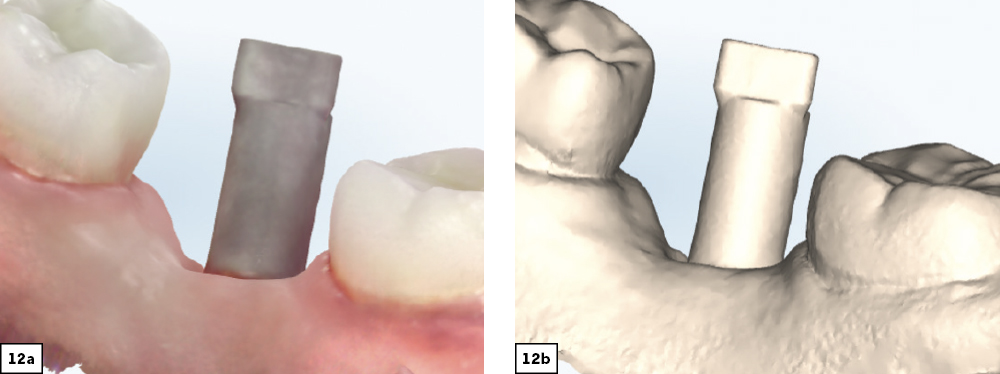
The Scan Body
Restorative Options
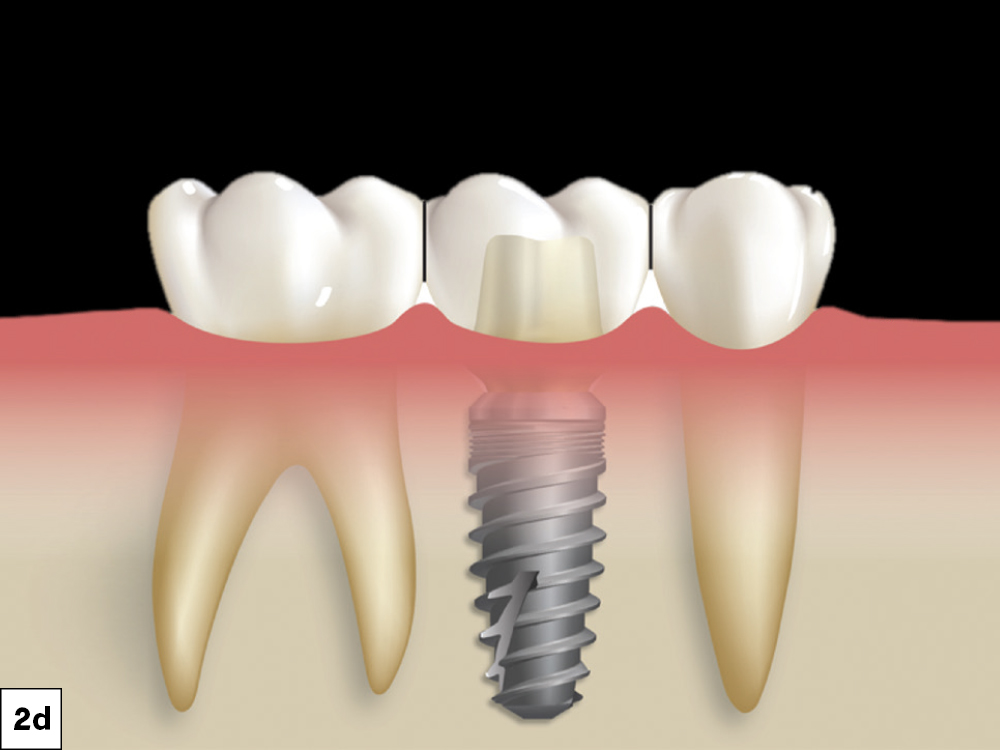
The restorative options available with digital impressions are similar to those from conventional impressions, including screw-retained crowns and custom abutments with cement-retained crowns. However, current intraoral scanning technology has certain limitations, including potential scan errors caused by implant angulation, the distance between multiple implants, and technical software and hardware difficulties that can lead to incomplete or distorted scans.2,3,4 Due to these limitations, an intraoral scan with scan bodies is recommended for single-unit or short-span implant restorations. As with all digital impressions, it is highly recommended to follow the specific scanning protocol for your intraoral scanner when acquiring a digital impression.5,6
Obtaining Accurate Digital Impressions






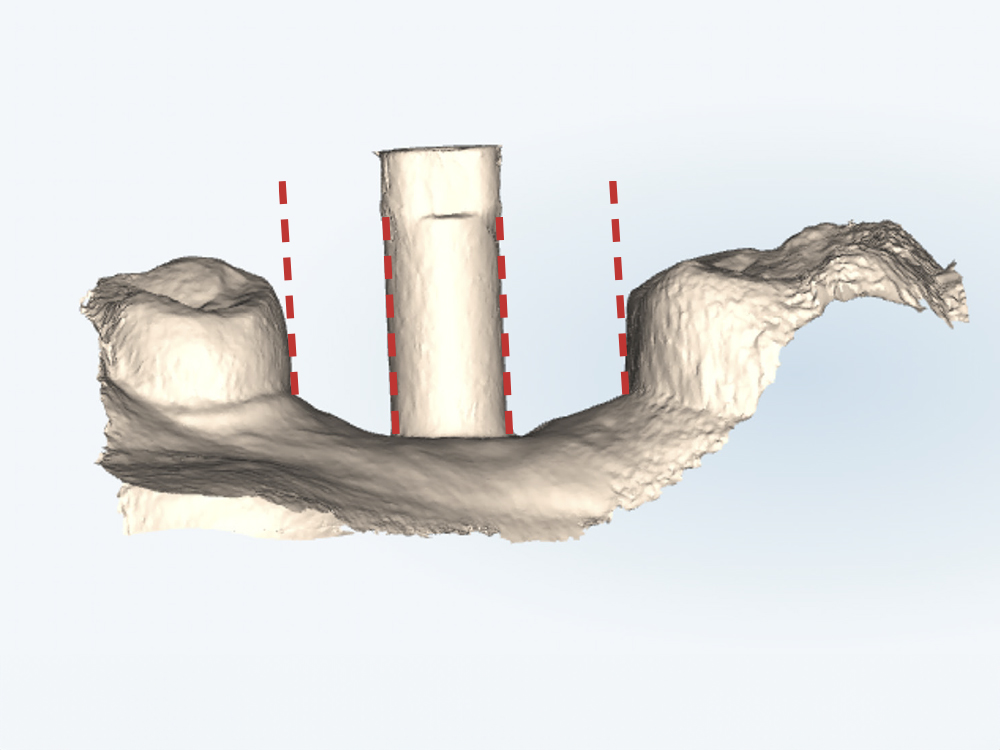
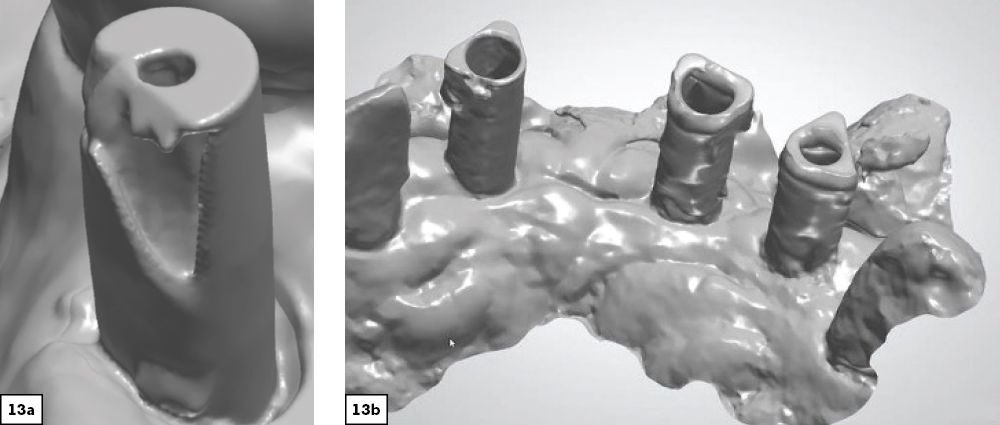
Take An Implant Scan

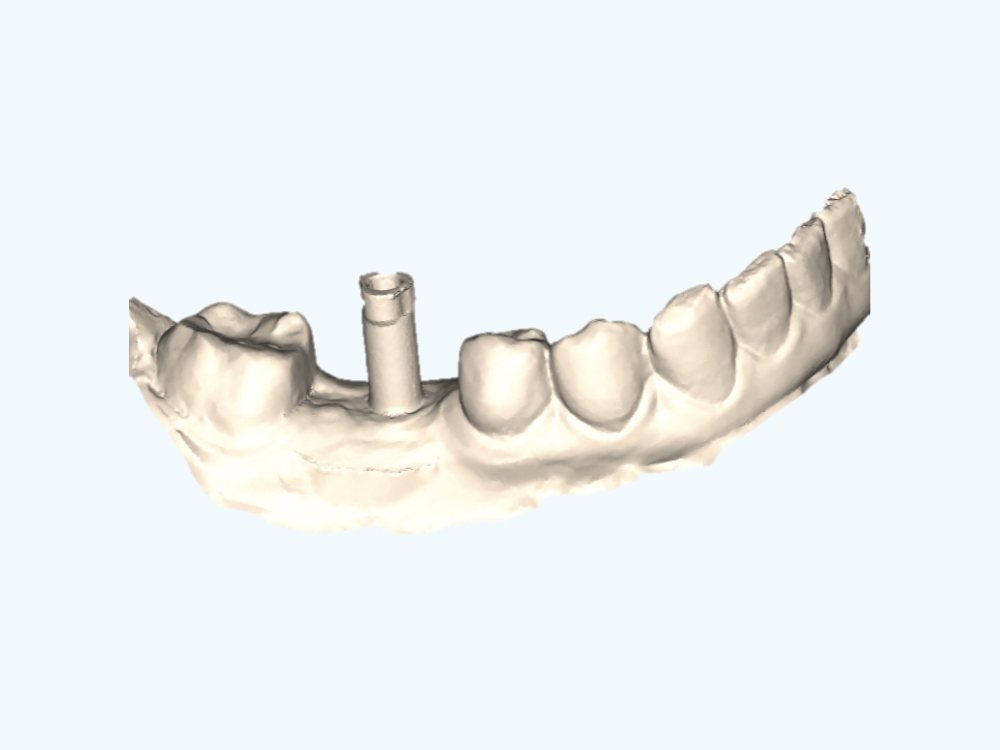
Scan The Implant Arch And The Opposing Arch

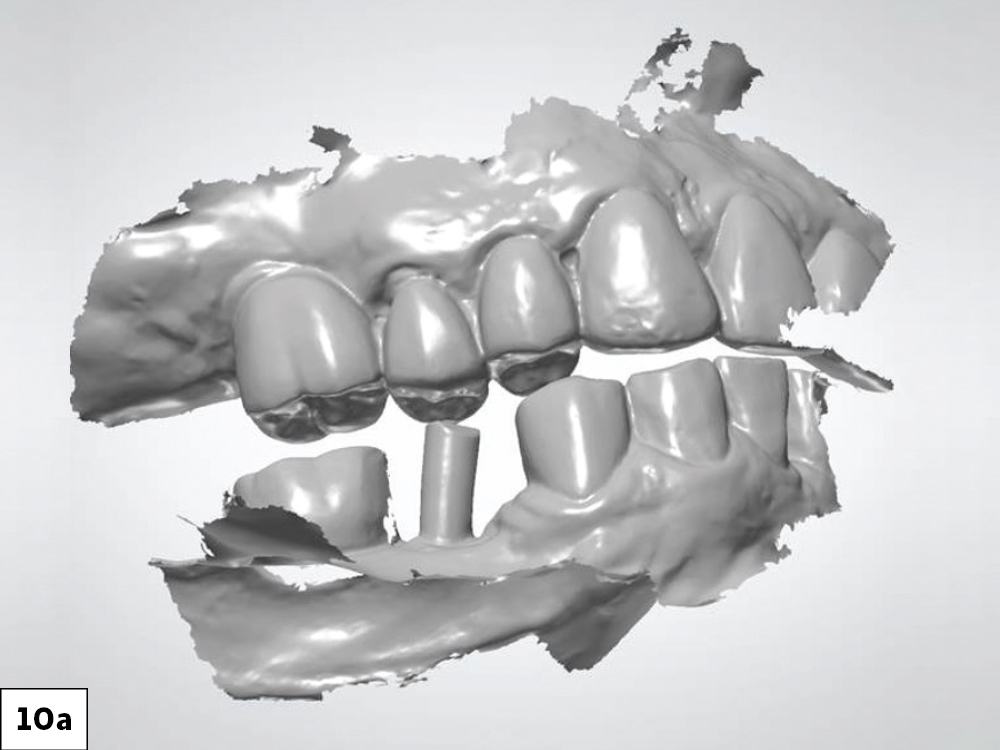
Scan The Bite

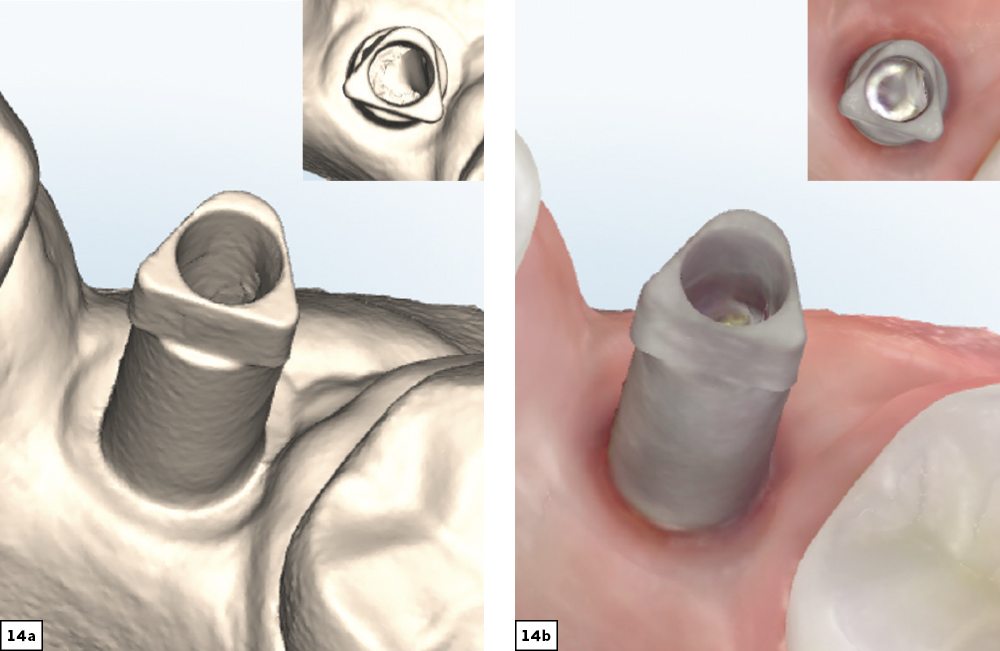
Evaluate Scan Quality

CONCLUSION
The use of digital impressions with implant cases makes it easier for the lab to provide a precise, well-fitting restoration with little discomfort to the patient. Plus, when doctors restore their digital cases with Glidewell, they receive everyday discounts on model-free custom abutments and screw-retained crowns. Following a straightforward scanning workflow will lead to more efficient lab communication and better restorative outcomes.
Available CE Course
References
-
Mizumoto RM, Yilmaz B. Intraoral scan bodies in implant dentistry: a systematic review. The J Prosthet Dent. 2018. 120(3):343-352.
-
Revilla-León M, Smith Z, Methani MM, Zandinejad A Özcan, M. Influence of scan body design on accuracy of the implant position as transferred to a virtual definitive implant cast. J Prosthet Dent. 2021.(6):918-923.
-
Choi Y-D, Eun Lee K, Mai H-N Lee D-H. Effects of scan body exposure and operator on the accuracy of image matching of implant impressions with scan bodies. J Prosthet Dent. 2020. 124(3): 379.e1-379.e6.
-
Revell G, Simon B, Mennito A,Evans ZP, Renne W, Ludlow M Vág J. Evaluation of complete-arch implant scanning with 5 different intraoral scanners in terms of trueness and operator experience. J Prosthet Dent. 2022. 128(4):632-638.
-
Papaspyridakos P, Vazouras K, Chen Y-W, Kotina E, Natto N, Kang K, Chochlidakis K. Digital vs conventional implant impressions: a systematic review and meta analysis. J Prosthodont. 2020. 29(8):660-678.
-
Schmidt A, Wöstmann B, Schlenz MA. Accuracy of digital implant impressions in clinical studies: a systematic review. Clin Oral Implants Res. 2022. 33(6):573-585.